



INTRODUCTION
Bleeding control is a crucial aspect of nasal surgical procedures, such as endoscopic sinus surgery (ESS) and rhinoplasty, due to the limited surgical field of view. Various techniques, including tranexamic acid, cauterization, and blood pressure reduction have been used to achieve clear visibility for the surgeon [1].
However, these methods have potential complications, such as direct mucosal damage from cauterization, and serious adverse effects, including cardiac ischemia, delayed recovery, rebound hypertension, emboli in the cerebral circulation, and permanent brain damage from blood pressure reduction [2,3]. The use of desmopressin, a synthetic form of the human hormone arginine vasopressin, has been suggested as a potential solution to reduce or even avoid the adverse effects of bleeding during nose surgery.
Desmopressin increases the levels of factor VIII and von Willebrand factor, which are released from endothelial cells, making it an effective treatment for hemophilia A and von Willebrand disease. Furthermore, previous studies have suggested that desmopressin can lower the transfusion rate in cardiac surgery [4,5]. Considering the beneficial effects of desmopressin on bleeding tendency, we conducted a meta-analysis to investigate the utility of desmopressin in nose surgery, building on the findings of several recently published papers that have described its effectiveness.
METHODS
Our institution does not require Institutional Review Board (IRB) approval for systematic review and meta-analyses based exclusively on published literature.
Search strategy and study selection
Clinical studies published in English prior to February 2023 were identified from PubMed, Scopus, Google Scholar, Embase, and the Cochrane Register of Controlled Trials. The following search terms were used: “desmopressin,” “chronic sinusitis,” “endoscopic sinus surgery,” “rhinoplasty,” “bleeding,” “operative field,” “operative time,” “satisfaction,” and “adverse effect.”
In this study, two independent reviewers screened the titles and abstracts of potential studies, excluding those that did not focus on the preoperative administration of desmopressin. When it was not possible to determine eligibility from the abstract alone, a full-text review was performed on studies deemed potentially relevant. Randomized controlled trials examining the perioperative administration of desmopressin in patients undergoing ESS or rhinoplasty were considered for inclusion, regardless of the administration route. Studies were excluded if they involved procedures other than sinus surgery or rhinoplasty, contained duplicate reports, or failed to present relevant outcomes with quantifiable data that could be evaluated from the published results. Fig. 1 outlines the search strategy utilized to select the studies for the meta-analysis. The review protocol has been registered with the Open Science Framework (https://osf.io/6qdpx/)
Data extraction and risk of bias assessment
Data from eligible studies were extracted using a standardized form and then reviewed by two independent reviewers to ensure accuracy and consistency [6]. The primary perioperative outcomes measured included intraoperative blood loss, operation time, and the quality of the surgical field, as evaluated by the 5-point or 10-point scores developed by Boezaart et al. [7,8] Additionally, secondary outcomes were collected, which encompassed measures of hemodynamic stability such as arterial blood pressure and postoperative serum sodium levels, surgeon satisfaction scores rated on a 5-point Likert scale, and side effects. Analyses compared the aforementioned outcomes between the treatment group, who received desmopressin, and the control group, who either received no treatment or saline administration during both the operation and the postoperative period.
We extracted data from the studies included in the analysis for several variables, including the number of patients, scores related to the quality of the surgical field and surgeon satisfaction, operative time, amount of intraoperative bleeding, occurrence of side effects, and the p-values reported for comparisons between the treatment and control groups [7-15]. This was done to determine the influence of desmopressin on intraoperative bleeding and other morbidities.
Statistical analysis
Statistical analysis of the quantitative variables from the included studies was conducted using the R program (Ver. 3.6.1; R Foundation for Statistical Computing, Vienna, Austria). The standardized mean difference (SMD) was employed as the summary statistic to normalize the results of different studies to a common scale when evaluating the same outcome measured by various methods. This approach facilitated the analysis of several parameters: the quality of the surgical field and surgeon satisfaction scores, the amount of operative blood loss and duration of surgery, intraoperative arterial blood pressure, and postoperative serum sodium levels. To detect potential publication bias, we utilized both a funnel plot and Egger’s test. Additionally, we applied Duval and Tweedie’s trim-and-fill method to adjust the overall effect size in light of publication bias.
RESULTS
All nine studies [7-11,13-16] included in this meta-analysis were randomized controlled trials (RCTs). Two of the articles were written by the same authors, but the research periods did not overlap. In total, 588 participants were included in the study, of whom 297 received desmopressin (treatment group) and 291 received normal saline spray or NaCl injection (control group). Desmopressin was administered as a nasal spray in five studies and intravenously in four studies. The study characteristics are presented in Table 1, and the results of bias evaluations are shown in Supplementary Table 1 (in the online-only Data Supplement). Publication bias was not analyzed because the nine trials included in the analysis were not sufficient to generate a funnel plot.
Effect of perioperative desmopressin on outcome variables
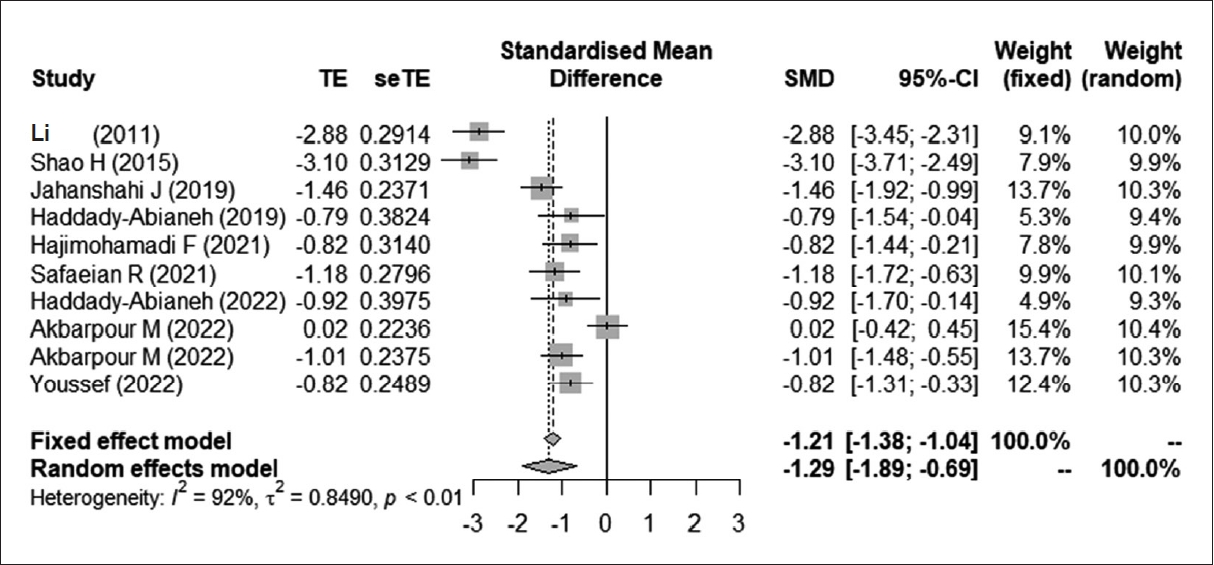
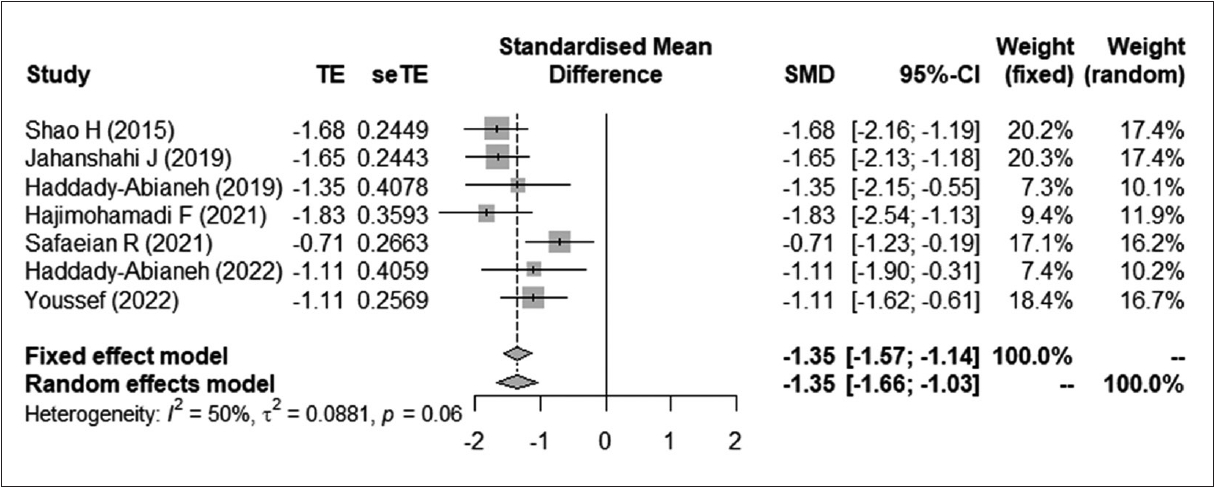
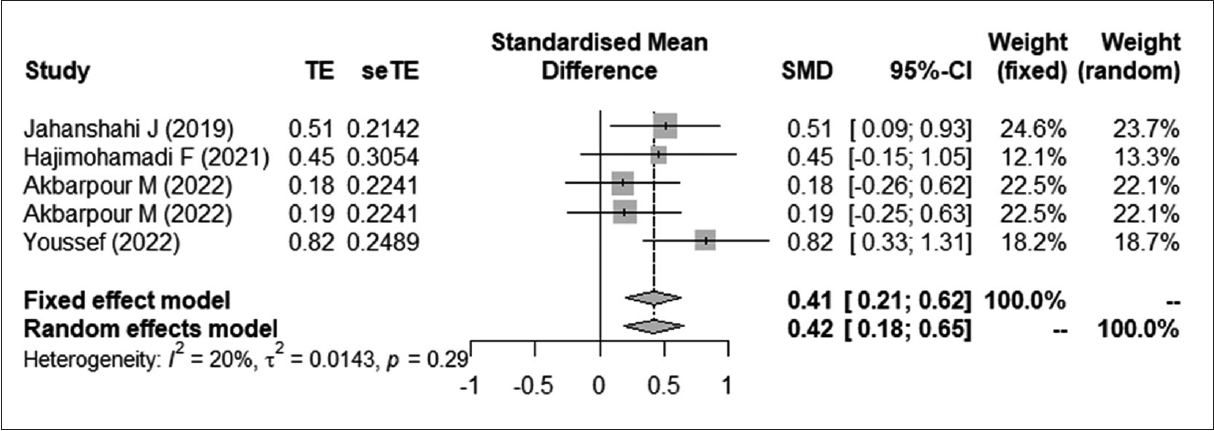
Intraoperative bleeding (SMD=-1.2946; 95% CI, -1.8944 to -0.6948; I2 =91.6%) was significantly lower in the treatment group than in the control group (Fig. 2). The quality of the operative field (SMD=-1.3496; 95% CI, -1.6643 to -1.0350; I2 = 50.3%) (Fig. 3) and surgeon satisfaction (SMD=0.8738; 95% CI, 0.4941 to 1.2534; I2 =0.0%) were significantly higher in the treatment group than in the control group (Fig. 4). Perioperative desmopressin showed a non-statistically significant association with shorter operative time (SMD=-0.4820; 95% CI, -0.9933; 0.0292; I2 =89.8%) (Fig. 5). There were no reported clinically significant adverse effects, but the treatment group had significantly higher values for intraoperative blood pressure (SMD=0.4136; 95% CI, 0.2052 to 0.6219; I2 =20.0%) (Fig. 6) and decreased postoperative serum sodium levels (SMD= -0.2393; 95% CI, -0.4465 to -0.0320; I2 =47.2%) than the control group (Fig. 7). Operative time, intraoperative bleeding, and the quality of the operative field showed significant interstudy heterogeneity (I2 >50%).
The overall analysis did not consider the desmopressin route (transnasal vs. intravenous) or surgery type (ESS vs. rhinoplasty). This omission is due to the high heterogeneity (more than 50%) of some results obtained by all studies. Six studies applied desmopressin in patients with chronic rhinosinusitis and three studies enrolled patients undergoing rhinoplasty. In a subgroup analysis according to the surgery type, the effect sizes did not differ considerably depending on the surgery type, and desmopressin showed a statistically significant effect on arterial blood pressure, operative bleeding, the quality of the operative field, and surgeon satisfaction. Although the rhinoplasty subgroup showed significantly lower postoperative serum sodium levels compared to the ESS subgroup (p = 0.0097), only one study was included for rhinoplasty; therefore, this result should not be overinterpreted (Table 2).
Five studies administered desmopressin through the transnasal route, while the other four injected desmopressin via the intravenous route. In a subgroup analysis regarding the administration route, the effect size did not differ considerably, and desmopressin use continued to have a statistically significant effect on arterial blood pressure, operative bleeding, the quality of the operative field, and operative time. Although the difference in postoperative serum sodium levels between the two subgroups was not statistically significant (p=0.0550), the intravenous subgroup had a significant effect on serum sodium levels, whereas the transnasal subgroup did not exhibit this effect. These findings suggest that surgeons should monitor serum sodium levels during systemic administration. No severe adverse effects, including significant hemodynamic instability or thromboembolic events related to the procedure, were reported.
DISCUSSION
The main finding of this study was that desmopressin is both statistically and clinically effective in reducing intraoperative bleeding, clarifying the operative field, and increasing surgeon satisfaction compared to the control group. Although desmopressin was not associated with any significant adverse effects, there were statistically significant increases in intraoperative arterial blood pressure and decreases in postoperative sodium levels; however, these changes were not deemed clinically significant. In light of our findings, we conclude that the administration of desmopressin prior to nasal surgery can significantly and favorably impact operative bleeding, making it an effective option for improving surgical outcomes in this setting.
Surgery can induce fibrinolysis due to surgical trauma, blood loss, consumption of coagulation factors, and administration of crystalloid fluids during and after surgery [17]. Desmopressin is a V2 analog of arginine vasopressin that releases von Willebrand factor and factor VIII from endothelial cells, which are essential for primary hemostasis. Von Willebrand factor binds to platelets and enhances platelet adhesion and aggregation, leading to the formation of platelet plugs, while factor VIII promotes the coagulation cascade [18]. A previous systematic review dealing with functional endoscopic sinus surgery (FESS) reported findings consistent with our study, supporting our finding that the desmopressin group had significantly better intraoperative bleeding control and surgical field clarity [12].
Although two RCTs reported that the desmopressin group tended to have decreased mean arterial pressure and heart rate, albeit without clinical significance [7,14], we found that intraoperative arterial blood pressure was statistically significantly higher in the desmopressin group than in the control group; nonetheless, this difference was also clinically insignificant. Safaeian et al. [14] controlled the acute increase in mean arterial pressure with incremental boluses of intravenous labetalol, and Shao et al. [7] showed that the acute increase in mean arterial pressure could be managed with intravenous remifentanil, esmolol, and nicardipine, potentially indicating that those agents could countervail or exceed the hypertensive effect of desmopressin. Given that anesthesiologists aim to control blood pressure, and considering the observed high blood pressure even with such control, it is plausible that desmopressin may contribute to an increase in blood pressure. However, further studies that control for blood pressure variables are warranted.
The effective dose of desmopressin is 0.3 μg/kg by intravenous infusion 30 minutes prior to the procedure or 1.5 mg/mL with one spray intranasally [19]. To the best of our knowledge, no previous study has compared the effects of desmopressin based on the administration route. We found that both intravenous and intranasal administration had significantly beneficial effects on operative bleeding and the operative field, and there were no statistically significant differences in desmopressin efficacy between the two routes of administration.
The most common adverse effect of desmopressin is hyponatremia, which can be either asymptomatic or symptomatic [20]. In this study, no significant differences were observed in the incidence of hyponatremia based on the route of administration. However, the intravenous route was associated with significant hyponatremia, whereas the intranasal route was not. Given the balance of beneficial and adverse effects of desmopressin, the intranasal route appears to be the preferred option in clinical practice.
We found that desmopressin is useful in both ESS and rhinoplasty groups in terms of reducing operative bleeding and increasing surgeon satisfaction. While a previous study has recommended the use of desmopressin in ESS, a meta-analysis evaluating its beneficial or adverse effects in rhinoplasty has yet to be conducted. Rhinoplasty is among the most common, delicate, and challenging plastic surgeries performed worldwide, making excellent surgical visibility a critical requirement. Our results suggest that desmopressin can assist surgeons by providing clearer operative fields through reduced bleeding, which in turn may lead to improved patient outcomes, including less ecchymosis and edema [10]. However, it is important to note that sodium levels were significantly lower in the rhinoplasty group than in the ESS group.
Our study had some limitations. First, variables such as patient baseline characteristics, preoperative medication or management, and surgeon skill could have influenced the results. This issue may account for the observed high heterogeneity. Nevertheless, we included only randomized controlled trials in our meta-analysis to improve the quality of the studies, despite the presence of several trials (case series or case-controlled trials) that reported varying results regarding the effect of desmopressin. Most meta-analyses adhere to strict criteria, such as the requirement for randomization and blinding in clinical trials, regardless of the variety of study types. Thus, our methodology, with its inclusion criteria, was beneficial in controlling bias and enhancing quality. Second, all study participants were from China or Iran. Since external or internal nasal anatomy can vary at the skeletal level, there is a need for generalized results that account for these differences. We endeavored to broaden the scope of important endpoints reported by all RCTs, such as hyponatremia and intraoperative hypertension, to strengthen the power of the pooled conclusions.
Our findings suggest that the perioperative administration of desmopressin in nasal surgery may have a positive impact on intraoperative bleeding, the surgical field, and surgeon satisfaction, regardless of the type of surgery or administration route. However, considering the adverse effects of desmopressin, including hyponatremia, that are associated with intravenous administration, we suggest that the intranasal route is preferable in clinical practice.
CONCLUSION
This study demonstrated that prophylactic treatment with desmopressin for nasal surgery effectively reduced intraoperative bleeding, resulting in an improved surgical field and increased surgeon satisfaction. Additionally, desmopressin was not associated with significant adverse effects, although mild hyponatremia and hypertension were observed. However, due to the potential for postoperative blood pressure elevation, the use of desmopressin should be carefully considered in patients with cardiopulmonary issues, and the intranasal route is recommended for clinical applications.




 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement
Supplement Print
Print






