



INTRODUCTION
Allergic rhinitis (AR) is a common chronic condition with a steadily increasing prevalence [1]. AR symptoms can greatly impact a patientŌĆÖs quality of life and may increase the risk for several diseases [2,3]. Medical therapy, including oral antihistamines, decongestants, and topical steroids, is the firstline treatment for relieving AR symptoms [4]. However, patients who are resistant to medications may benefit from surgical interventions aimed at relieving symptoms [5]. Turbinoplasty, a surgical procedure to reduce the inferior turbinate (IT), can be used to treat nasal obstruction caused by turbinate hypertrophy. During surgery, the mucosa, soft tissue, and turbinate bone are removed. Techniques used to widen the nasal airway by reducing the IT volume include conventional, laser, cryo-, and electrocautery turbinectomy; conventional turbinoplasty; and microdebrider- or coblator-assisted turbinoplasty [6].
Although these surgical techniques yield satisfactory outcomes, unfavorable side effects such as epistaxis, crustation, unpleasant odors, and IT atrophy are frequently observed postoperatively [7]. Theoretically, turbinoplasty, which widens the nasal cavity, should minimize complications while improving the patientŌĆÖs symptoms [8]. Among various turbinoplasty approaches, radiofrequency ablation and microdebrider-assisted turbinoplasty commonly cause coagulative necrosis, which eventually degrades the hypertrophic edematous volume while conserving the mucosa. Microdebrider-assisted turbinoplasty is a minimally invasive method for reducing IT size and maintaining mucosal integrity. It has the advantages of a short healing time, mild decrease in mucociliary clearance, minor postoperative complications, and good functional outcomes. In coblator-assisted turbinoplasty, a relatively low temperature (40┬░CŌĆō100┬░C) is produced by bipolar radiofrequency, resulting in fibrosis of the submucosal tissue. This fibrotic change leads to a widened nasal cavity and destroys the vascular structure and glands in the submucosal layer, resulting in the restriction of allergic reactions [7,8].
This study compared the long-term clinical outcomes of microdebrider- and coblator-assisted turbinoplasty.
METHODS
Patient enrollment
This retrospective study was approved by the Institutional Review Board of Dankook University Hospital (IRB No. 2022- 09-022). The patientŌĆÖs consent was waived by the IRB approval. A total of 342 patients diagnosed with AR based on allergy tests such as the multiple allergen simultaneous test (MAST), skin prick test (SPT), or ImmunoCAP┬« test and who underwent treatment for AR between January 2010 and June 2017 in a tertiary referral hospital, were initially recruited. Patients with a severely deviated nasal septum, a short follow-up period (<4 years) after treatment, other sinonasal inflammatory disease such as chronic rhinosinusitis, or a history of previous nasal surgeries (septoplasty or endoscopic sinus surgery) were excluded. Finally, 241 patients (179 males and 62 females) aged 4 to 73 years (mean 25.3┬▒13.6 years) were enrolled in this study. Patients were divided according to surgical technique into microdebrider and coblator groups.
PatientsŌĆÖ clinical course
Diagnosis of AR
Allergy tests were performed using the common 50 allergens. All tests and readings were performed by experienced personnel.
To calculate the mean for each allergen, testers measured the largest diameter of the wheal and the diameter orthogonal to it. A mean wheal width greater than or equal to that of histamine (positive control) was considered a positive reaction. Saline controls were all negative. Patients were considered allergic if at least one SPT result for any of the allergens tested was positive [9]. Patients who were too young for SPTs or who were taking medication that might affect the SPT reaction underwent MAST or ImmunoCAP® testing.
Patient serum was introduced to MAST pette chambers (MAST Systems, San Diego, CA, USA) containing 30 different types of allergens to perform the MAST. Anti-IgE with an enzyme tag was added after 2 hours of incubation and washing. The luminescent reagent was added after an additional 2 hours of incubation and washing. Using a MAST Optigen luminometer (Hitachi Chemical Diagnostics Inc., Mountain View, CA, USA), the results were categorized into classes 0ŌĆō4 after incubation (10 minutes). Classes Ōēź2 were considered positive [10].
Preoperative ImmunoCAP┬« testing (Thermo Fisher Scientific/Phadia┬« AB, Uppsala, Sweden) was performed according to the manufacturerŌĆÖs instructions. The instrument was utilized, and Dermatophagoides pteronussinus, Dermatophagoides farinae, mold mix, tree mix, grass mix, and weed mix were the six categories of allergens present. In cases of D. pteronussinus and D. farinae, test findings were divided into classes from 0 to 6 kUA/L, with class 2 read as AR. Test outcomes for the remaining four allergens were categorized as either positive or negative. AR was also identified in patients with more than one positive test result.
Medical treatment and surgery
Leukotriene antagonists, intranasal steroid sprays, and antihistamines were used during medical treatment in accordance with the guidelines published by Bro┼╝ek et al. [11].
When medical treatment failed to alleviate symptoms and discomfort, surgical intervention with turbinoplasty was performed. Patients who consented to turbinoplasty underwent either coblator-assisted turbinoplasty or microdebrider-assisted turbinoplasty, as determined by the surgeon during the surgical procedure. All were inpatient procedures with the patient under general anesthesia and local submucosal anesthesia of the turbinates (2% lidocaine + 1:100,000 epinephrine; 5 mL syringe with a 1.5-inch, 27-gauge needle). The field of vision was secured using a nasal endoscope.
Microdebrider-assisted turbinoplasty
At the anteroinferior end of the IT, a mucosal incision was made with a no. 15 blade to establish a 0.5ŌĆō1.0 cm window. Using a Freer elevator, a submucosal tunnel was made along the turbinateŌĆÖs length. The submucosal tissue was then removed using a suction irrigation system, while a straight microdebrider blade with three diameters (Stryker TPS, Stryker Instruments, Kalamazoo, MI, USA) was introduced along the tunnel, decreasing the volume of the hypertrophied IT (4,000ŌĆō5,000 circulations/second). Extra care was taken to keep the mucosa intact. Using a cautery and nasal pack, bleeding was controlled.
Coblator-assisted turbinoplasty
The turbinates were assessed, and an electrode was inserted at an appropriate location. The electrode was only inserted once or twice to prevent damage to the nasal mucosa. A bipolar radiofrequency needle electrode with an active electrode diameter of 1 mm and shaft length of 10 mm (Smith & Nephew Arthrocare Corporation, London, UK) was inserted into the submucosal layer of the anteromedial and posteroinferior sides of the anterior IT (Fig. 1). Using a coblator wand, the entire lateral aspect of the interior turbinate mucosa and soft tissue was removed in a posterior to anterior direction. Alternate orientations of the coblator wand could be selected by the operator. The inserted coblator wand was activated using an ablation pedal at a grade 4 power level for 6ŌĆō10 seconds. Immediate shrinkage of the submucosal tissue was observed.
Symptom questionnaires, overall satisfaction, and medication scores
Using a numerical rating scale, nasal and AR symptoms including nasal blockage, rhinorrhea, sneezing, and itching were assessed. The 5-year postoperative symptom scores were obtained by telephone surveys, while the preoperative symptom scores were assessed using questionnaires at the initial visit.
The presence of surgery-related complications (complication or no complications), changes in medication scores (1=increased, 2=no change, 3=decreased, and 4=not using medication), and subjective patient satisfaction scores (1=unsatisfied, 2=neutral, and 3=very satisfied) were all obtained via telephone surveys.
Data analysis and statistics
The treatment outcomes of the microdebrider and coblator groups were compared based on postoperative 5-year follow-up results. Changes in the degree of AR symptoms (nasal obstruction, rhinorrhea, sneezing, and itching), medication treatment from preoperative to 5 years postoperative, and satisfaction with the procedure were prospectively compared between the two surgical methods.
Data for patients <18 years old were obtained from their caregivers. Results were expressed as mean┬▒standard deviation. Paired or unpaired t-tests and repeated-measures analysis of variance were applied as indicated and all analyses were performed using GraphPad Prism software version 5.03 (GraphPad Software, Inc., San Diego, CA, USA). Statistical significance was set at p<0.05.
RESULTS
Demographic and clinical characteristics of patients
Of the 241 patients included in the study, 192 and 49 underwent microdebrider- or coblator-assisted turbinoplasty, respectively. Although the mean age at diagnosis was significantly different between the groups (26.4┬▒14.8 vs. 27.1┬▒11.73), no significant differences were observed in the sex ratio (microdebrider group: 71.3% male vs. coblator group: 85.7% male) or initial symptom scores preoperatively. Characteristics of the study population are presented in Table 1.
Treatment outcomes of the microdebrider and coblator groups
Allergic symptom scores
There were no statistically significant differences between the microdebrider and coblator groups in all four nasal symptom scores, both preoperatively and postoperatively. At the 5-year follow-up, the mean scores for all four symptoms improved significantly in both groups. In the microdebrider group, postoperative nasal obstruction (6.02┬▒2.93 to 3.82┬▒2.90), rhinorrhea (5.10┬▒3.13 to 3.27┬▒2.70), sneezing (4.25┬▒3.13 to 2.69┬▒2.74), and itching (3.52┬▒3.34 to 1.88┬▒2.53) improved significantly. Patients in the coblator group had significant improvements in nasal obstruction (6.57┬▒2.58 to 3.84┬▒2.55), rhinorrhea (5.18┬▒3.08 to 3.22┬▒2.64), sneezing (5.18┬▒2.86 to 2.49┬▒2.36), and itching (4.57┬▒2.92 to 2.37┬▒2.60) after surgery (all p<0.0001). No statistically significant differences were observed in the degree of symptom improvement between the microdebrider and coblator groups (Fig. 2).
Postoperative medication and subjective satisfaction scores
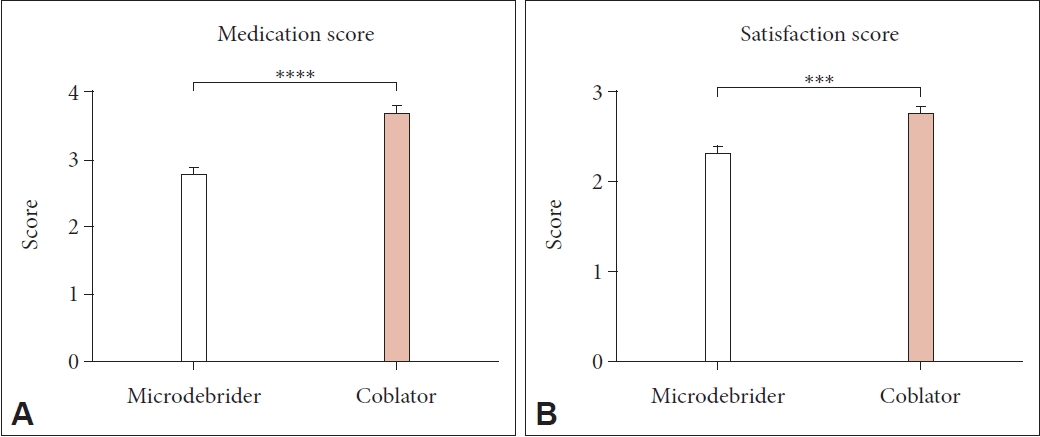
At the postoperative 5-year follow-up, the coblator group showed significantly improved medication scores compared with the microdebrider group (p<0.0001). The mean medication score of patients in the coblator group was 3.69┬▒0.61, while the mean score of patients in the microdebrider group was 2.79┬▒0.96 (Fig. 3A). Furthermore, patients in the coblator turbinoplasty group had significantly higher overall satisfaction scores than those in the microdebrider group at the 5-year follow-up. The mean satisfaction score of patients in the coblator group was 2.76┬▒0.43, while the mean score of patients in the microdebrider group was 2.32┬▒0.73 (p=0.0001) (Fig. 3B).
DISCUSSION
AR is a highly prevalent condition that affects millions of patients each year, and the defining symptom of nasal obstruction has a substantial influence on quality of life. There are numerous surgical treatments for AR, most of which are aimed at the underlying nasal obstructive component [12].
Medical management is the first-line treatment for nasal obstruction caused by turbinate hypertrophy; however, turbinates refractory to medical management are treated surgically [6,13]. Oral, intranasal, or ocular H1-antihistamines, intranasal corticosteroids, or a set mix of intranasal H1-antihistamines and corticosteroids are the most commonly used medications [14]. In patients with persistent symptoms, allergen immunotherapy administered by a specialist using high-quality extracts has been shown to be useful [15].
If symptoms such as nasal congestion do not improve despite these pharmacological treatments, an otolaryngologist may recommend surgery [16]. Surgical management can be broadly classified into radical or conservative procedures [17,18]. Radical procedures include total or partial turbinectomy, while conservative procedures are grouped into submucosal resection, coblation, and laser- or microdebrider-assisted turbinoplasty [19]. Bleeding and mucosal damage are the two major disadvantages of radical procedures [6]. Conservative procedures, mainly submucosal turbinoplasty, preserve the mucosa and result in minimal morbidity [20,21].
This study confirmed the long-term efficacy of two different surgical methods of turbinoplasty. Both methods were clinically effective, and the choice of power instruments was dependent on the personal and clinical preferences of the surgeons [22].
The results of this study support the findings of other recent prospective investigations that found that the type of surgical method (microdebrider or coblator) did not have a significantly different effect on the relief of AR symptoms [23]. However, itching and sneezing are generated when the trigeminal afferent nerve, which supports nociceptive sensory responses in nasal mucosa, is activated. These itch-sensing nociceptors have terminal branching with thin axons. Therefore, it is possible that turbinate volume reduction using the radiofrequency coblator has a more significant effect on decreasing the superficial surface area available for allergen contact, or that the energy transduction that destroys submucosal vessels, glands, and nerve fibers is more powerful than microdebridement [24]. In this study, patients who received coblator-assisted turbinoplasty had higher postoperative satisfaction and used less medication following surgery. The mechanism described above may explain some of these results.
This study had some limitations. It is important to acknowledge that the choice of surgical procedure (coblator-assisted turbinoplasty or microdebrider-assisted turbinoplasty) in our study was made based on the surgeonsŌĆÖ judgement during the surgical procedure. This approach may introduce a selection bias since various factors, such as the patientŌĆÖs anatomical characteristics or intraoperative conditions, could influence the surgeonŌĆÖs decision. Future research is needed to explore the impact of these factors on surgical procedure selection to better understand their potential effects on outcomes. The patientsŌĆÖ long-term follow-up status was evaluated based on subjective symptom and satisfaction scores obtained via telephone surveys, thus affecting the objectivity of the study. Moreover, the long-term follow-up period of the study was only 5 years, a subjective choice made by the authors. In addition, this study did not measure the exact changes in nasal airway volume or IT reduction before or after surgery, because the study was based on subjective data. Therefore, further studies with larger sample sizes and longer postoperative follow-up periods are required to evaluate patientsŌĆÖ objective and subjective status. Numerical measurements or analyses of hypertrophic turbinates using imaging studies will be helpful for identifying patients with relapse or symptom recurrence. In addition, we recommend further research to investigate the pathophysiology of the different submucosal methods, which may be helpful for selecting surgical methods based on the different disturbances or symptom manifestations in patients. Another limitation of our research was our inability to examine the potential complications linked to turbinoplasty, including bleeding, nasal dryness, and symptoms indicative of empty nose syndrome. While our study helped clarify the effectiveness of both surgical methods, further studies are needed to investigate the occurrence and potential disparities in complication rates between these two modalities.
This long-term follow-up study showed that radiofrequency-assisted turbinoplasty is as effective as microdebrider-assisted turbinoplasty for relieving nasal symptoms and improving medication scores in patients with AR. Thus, the coblator can be considered the equipment of choice for AR patients since the coblator-assisted turbinoplasty group showed better long-term outcomes in terms of medication scores and overall satisfaction scores. The authors plan to conduct randomized controlled trials (RCTs) with a larger cohort of patients in our future research endeavors. Specifically, we intend to investigate significant outcomes such as long-term postoperative quality of life, patient-reported symptom relief, and complication rates between the two surgical modalities. Additionally, we will analyze subgroups to assess the impact of anatomical variations and other potential factors on treatment outcomes. These RCTs will provide a more comprehensive understanding of the comparative effectiveness and safety of coblator-assisted turbinoplasty and microdebrider-assisted turbinoplasty.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






