The YSK Olfactory Function Test: Development of a New Korean Olfactory Test
Article information

Abstract
Olfaction is an important aspect of quality of life, beyond simply smelling food and recognizing danger. Recently, research has focused on its association with various diseases, such as neurodegenerative diseases or viral infections. The evaluation of olfactory function must take into consideration the cultural experience of the target group. A new Korean culturefriendly olfactory function test, the YSK olfactory function test (YOF test, Kimex Co.), uses safe odorants, such as phenyl-ethyl alcohol (PEA) (not n-butanol), for the threshold test. Furthermore, odorants in the YOF identification test reflect each of eight major chemical functional groups. The diagnostic cut-off for anosmia was a Threshold Discrimination Identification (TDI) score of ≤14.5 and that for hyposmia was 14.5<TDI≤21.0. The YOF test showed relevant diagnostic validity for olfactory dysfunction when compared with the Korean version of the Sniffin’ Stick-II test. In this review, we share our experiences developing a new Korean-friendly olfactory function test.
INTRODUCTION
Olfaction is the sense of recognizing external chemical substances among the five human senses. Olfaction has long been underestimated in its importance as a chemical sense with a subjective aspect to cognition [1]. However, as the understanding of the physiological mechanism of smell increases, the importance of smell evaluation is also attracting attention. A decreased sense of smell can affect quality of life, such as depression and weight change, or even affect mortality. Additionally, it is expected to serve as a biomarker for early diagnosis of neurodegenerative diseases such as Parkinson’s and Alzheimer’s disease. Furthermore, studies have discovered the deposition of proteins related to the pathophysiology of dementia in the olfactory bulb [2–6]. Recently, as it has been known that a high rate of olfactory loss is found in a high percentage of patients infected with SARS-CoV-2, the evaluation of olfactory function has become especially important [7,8].
In this review, the characteristics of the newly developed YSK olfactory function test (YOF test, Kimex Co.) are introduced, and its future use is summarized. The data on the YOF test and the Korean version of the Sniffin’ Stick (KVSS-II) test mentioned in this review are derived from the development paper of the YOF test published in 2020 [9], and the sources for all other citations are specified.
Background of the YOF test
Olfactory function evaluation methods follow one of three forms [10]. The first is a subjective self-olfactory assessment of the test, such as the Visual Analogue Scale score or the Questionnaire of Olfactory Disorders score. The second is a psychophysical olfactory assessment, which scores a subject’s response to olfactory stimuli. It is more reliable than subjective self-evaluation and can be used to diagnose olfactory disorders. Tests for this assessment include the University of Pennsylvania Smell Identification Test (UPSIT), the Sniffin’ Stick test, and the Korean version of the Sniffin’ Stick test (KVSS-II), all of which are familiar to otolaryngologists. The third assessment objectively evaluates a subject’s response to olfactory stimulation using electrophysiological tests such as electroencephalography or electrooculography or using functional imaging tests (e.g., functional MRI). However, in clinical practice, psychophysical olfactory testing is the most widely used clinically because expensive equipment is rarely available in clinical settings and is still in the research stage.
The psychophysical olfactory test includes one or more odor thresholds, odor discrimination, and odor identification tests [10]. Because the subject’s exposure to the olfactory source significantly affects the perception of smell, the clinically used olfactory test must clarify the target group and consider the cultural aspect in selecting the odorants. For this reason, tests such as the Sniffin’ Stick test and UPSIT, which are currently the most widely used olfactory tests, have been modified for use in each country. Additionally, studies have been conducted to verify the effectiveness of the target population. KVSS-II, the most widely used olfactory test in Korea, is also a localized test of the Sniffin’ Stick test by modifying the identification test odorants and options. Since KVSS-II was developed in 1999, its reliability has been verified in olfactory evaluation for Koreans and has been widely used in clinical practice. However, in some papers that reported the correct rate for each item of the KVSS-II identification test in subjects with a normal sense of smell, three or more items had a very low correct rate (licorice, rosin, apple, etc.), suggesting the need for improvement [11,12].
The psychophysical test method inevitably requires human exposure to chemicals, as it is a test method that detects the smell of an olfactory source and scores the subject’s reaction. Caution is required in the clinical application that exposes the human body to such chemicals [13,14]. In particular, the experience of interstitial lung disease in children caused by humidifier disinfectants from 2006 to 2011 in Korea raised social awareness about the safety of chemicals used in the human body [15,16]. For this reason, it is necessary to exclude chemicals harmful to the human body as much as possible and to develop an olfactory test using chemicals whose safety has been verified for a long time.
The YOF test increases the effectiveness of the test by adopting odorants familiar to Koreans, along with universal odorants, regardless of the culture in consideration of the cultural experience of Koreans. A method including chemicals used in olfactory tests such as 2-phenyl-ethyl alcohol (PEA), which is used as a component for cosmetics with a floral scent, instead of n-butanol, which may cause inhalation toxicity as an odorant for threshold testing, was developed.
YOF test composition and test method
The YOF test consists of three categories of tests: olfactory threshold, identification, and recognition, as recommended in the positional paper on olfactory dysfunction published in 2016 (Fig. 1A) [10]. The YOF test contains odorants in a pentype container (Fig. 1B): the threshold and discrimination tests consist of three pens at each stage, and the olfactory recognition test consists of a single pen. When performing the test, the lid of the test pen is opened, and the patient is allowed to smell it for 3 seconds at a distance of 2 cm from the tip of the nose. Examiner should allow 30 seconds between each test step to avoid acclimatization to the olfactory stimulus. The examination room should be equipped with a hood or well-ventilated environment. In addition, to block visual information, the patient’s eyes should be covered with an eye patch during the test (Fig. 1C). When smelling different pens, even if the patient is hesitant to choose an answer due to a poor sense of smell, an answer must be selected during the test. Each olfactory threshold/identification/cognition test is given a score of 12 points (threshold test, 1–12 points; discrimination test and recognition test, 0–12 points each), and the person’s olfactory function is evaluated with a total of 1–36 points (Supplementary Fig. 1).

YSK olfactory function test kit. A: Exterior photo of the YSK kit. B: A testing pen that contains an odorant. When the lid is opened, the subject can smell the scent. C. The actual evaluation is being carried out under a well-ventilated hood.
YOF threshold test
The olfactory threshold is the concentration at which 50% of person detect the scent and 50% do not. In the olfactory threshold test, it is not necessary for subjects to distinguish scents or to identify which scent it is. Instead, the test checks whether the presence of olfactory stimulation can be recognized by concentration. The YOF olfactory threshold test uses rose-scented PEA that is commonly used in perfume. PEA, along with n-butanol, is the most widely used odorant for olfactory threshold testing. PEA has the advantage in that the olfactory stimulation is not unpleasant and does not stimulate the trigeminal nerve [17]. In several previous studies, the reliability and validity of the olfactory threshold test using PEA compared to that using n-butanol have been reported [18,19].
The YOF olfactory threshold test consists of a total of 12 steps, starting with 10% PEA at the highest concentration that is then diluted with a solvent of dipropylene glycol in a 1:2 ratio for each step. Each step consists of three pens (triplet test pens), one containing PEA and two pens containing solvent only. The subject remembers scent characteristics by smelling the highest concentration, the level 1 pen, for 3 seconds while blindfolded. At each level, subjects are instructed to choose a rose-scented pen among the three pens (three alternative-forced test). The clinician switches from the lowest concentration (level 12 pen) to the level 10 pen, then continues to switch to a pen of two levels higher until the subject gets the correct answer. If one is correct twice in a row, this becomes the first turning point, and the concentration goes down one level. This time, if one is correct twice in a row, it goes down another level. However, if one is incorrect even once, this level is the second turning point. In this way, for finding the odd-numbered (1, 3, 5, 7, etc.) level of pen, the turning point moves up by two levels until the answer is correct twice in a row. When looking for even-numbered (2, 4, 6, etc.) turning points, the concentration goes down one level until the answer is incorrect. The average score of the last four turning points out of a total of seven turning points becomes the olfactory threshold score (Fig. 2).
Example of scoring for YOF threshold test. The lowest concentration (level 12) goes up by two levels until patient gets the correct answer. If patient gets the right answer twice in a row (red double O), this becomes the first turning point and the concentration goes down one level. If patient gets the correct answer twice in a row (red double O), it goes down one level, and if patient gets the answer wrong even once (red O X or single X), this is the second turning point. In this way, finding the odd-numbered (1, 3, 5, 7, etc.) level of pen, the turning point goes up by two levels until the answer is correct twice in a row. When looking for even-numbered (2, 4, 6, etc.) turning points, go down one level until the answer is wrong. The average score of the last four turning points (in gray box) out of a total of seven turning points becomes the olfactory threshold score. The red double O symbol denotes the turning point going down. The red O X or single X symbol denotes turning point going up. YOF, YSK olfactory function.
YOF discrimination test
The YSK olfactory discrimination test consists of 12 steps, each with three pens containing one target odorant and two identical nontarget odorants. The subject smells all three test pens and then selects a target odorant that smells different from the other two. The total number of correct answers among the 12 steps is summed and evaluated. The composition of the target and nontarget odorants of the YSK olfactory identification test is shown in Table 1. Single chemicals, not complex chemicals, were selected and used as odorants. At each stage, the composition of target and nontarget scents was designed to easily match more than two-thirds of people with a normal sense of smell.

Odorants of the YOF discrimination test and correct answer rates for the normosmia group
YOF identification test
To select odorants to be used in the YSK olfactory perception test, 32 candidate odorants were evaluated in the development stage on 113 people (71 males, 42 females; mean age, 38.5 years) with a normal sense of smell. The sample size of 113 for this preliminary study was larger than in the preliminary studies of UPSIT (n=52) and Sniffin’ Sticks test (n=21) [20,21]. All candidate odorants were placed in a brown bottle and sniffed at a distance of 3 cm from the nose so that one answer out of four was correct. Of the 32 candidate odorants, 14 odorants yielded a correct answer rate of more than 90%. A total of 12 odorants were finally selected in consideration of the cultural familiarity and major chemical functional groups of the odorants. The odorants for the olfactory perception test consisted of eight culturally universal odorants and four Korean culture-friendly odorants. In addition, these 12 odorants represented eight major chemical functional groups (ketone, terpene, aldehyde, aromatic, alcohol, ester, acid, and amine) (Table 2). In the YSK olfactory recognition test, each subject was asked to smell the test pen at each level and choose the correct answer among four given answers. The sample items at each level were designed to reduce confusion so that subjects could easily choose if they smelled and recognized the scent normally (Table 3). Distractors can also affect the test results, and the need for improvement of the distractors in KVSS-II has been raised in a previous study [11]. Comparing to KVSS-II, the distractors of YOF identification test were relatively clear and easy to imaging the odors (e.g. curry, kimchi, etc.), not like some ambiguous distractors of KVSS-II (e.g. “coconut” against “walnut” in the same question or “glue,” “fir tree,” “cabbage”, etc.)
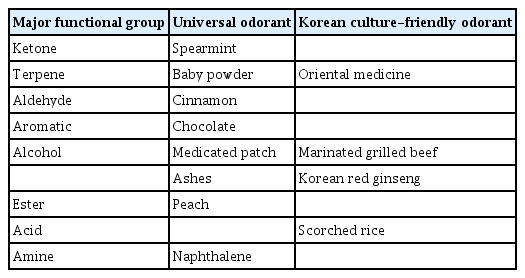
Composition of odorants for the YOF identification test

Odorants of the YOF identification test, their distractors, and correct answer rates for the normosmia group
DEMOGRAPHIC DATA OF YOF TEST USERS
We presented the results of an analysis of 1,127 patients who performed the YOF test and KVSS-II together at a single tertiary medical institution [9]. Subjects were divided into three groups through self-assessment: 542 people in normosmia group (335 males, 207 females), 472 people in hyposmia group (245 males, 227 females), and 113 people in anosmia group (54 males, 59 females) (Table 4). The mean age was the highest in hyposmia group at 52.9 years (standard deviation [SD], 14.1), followed by hyposmia group (mean, 49.6; SD, 16.3) and normosmia group (mean, 47.0; SD, 16.9); each group showed a statistically significant difference (p<0.001). It is well known that olfactory function decreases with age, and in the YOF test, age and Threshold Discrimination Identification (TDI) score (the sum of threshold, discrimination, and identification scores) showed a negative correlation (β=−0.115; R2=0.081; p<0.001). The TDI score of the YOF test and the threshold, discrimination, and identification scores were the highest in normosmia group, followed by hyposmia group and anosmia group; there was a statistically significant difference in the average scores between each group.

Demographic data and descriptive statistics for the YOF and KVSS-II test users by self-assessed olfactory function
Reliability of the YOF test
In the article of the development of YOF test, test-retest reliability was not suggested. To overcome this weak point, we additionally underwent the calculation of Cronbach’s alpha, which is the most common internal consistency reliability for single administration [22,23]. The Cronbach’s alpha of the YOF test from the data of original development article (n=1,127) was 0.768 which means acceptable.
Comparison of YOF test and KVSS-II results in normosmia group
The YOF test results in normosmia group showed good agreement with the KVSS-II results. The TDI score (r=0.86), as well as the threshold (r=0.57), identification (r=0.65), and cognitive (r=0.80) scores, of the YOF and KVSS-II tests showed a statistically significant correlation for each score (p<0.001). When comparing threshold, discrimination, and identification scores, the TDI score showed the highest correlation coefficient between the YOF and KVSS-II tests. This result is consistent with the previous report that the comprehensive evaluation of the TDI score is also more reliable than the separate evaluation of the threshold, discrimination, and identification scores [24].
The average results of the YOF test in normosmia group were as follows: the TDI score, 24.2 (SD, 4.5); the threshold test, 4.6 (SD, 2.3); the discrimination test, 8.6 (SD 2.1); and the identification test, 11.1 (SD, 1.7). The average results of the KVSS-II test in normosmia group were as follows: the TDI score, 30.4 (SD, 5.9); the threshold test, 6.8 (SD, 2.6); the discrimination test, 11.5 (SD, 2.7); and the identification test, 12.1 (SD, 2.3). Because the KVSS-II and YOF tests have different total scores of 48 and 36, respectively, it is difficult to judge that the YOF test simply has a low score. We compared the relative score distribution by dividing the YOF test and KVSS-II scores by their respective total scores (Fig. 3). In the YOF and KVSS-II tests, the TDI, threshold, and discrimination scores showed a relatively similar distribution. Still, the identification test showed a remarkably high trend in the YOF test. This is because the identification test of the YOF test was designed to make clear selections without confusion as long as one could smell the scent. On average, each question in normosmia group had a high percentage of correct answers (>90%).
Comparison of the score ratio (0 to 1, test score/score scale) between the YOF test and the KVSS-II test for the normosmia group. In the YOF and KVSS-II tests, the TDI, threshold, and discrimination scores showed a relatively similar distribution. The identification score showed a remarkably high trend in the YOF test. ***p<0.001. KVSS, Korean version of Sniffin’ Stick; YOF, YSK olfactory function; TDI, Threshold Discrimination Identification. Adapted from Ha et al. Clin Exp Otorhinolaryngol 2020;13(3):274–84 [9].
Setting the olfactory diagnosis score of the YOF test
The YOF test uses statistical methods (receiver operating characteristic curve and Youden’s J score) to score 1–14.5 for anosmia, 14.75–21.0 for hyposmia, and 21.25–36 for normosmia [9]. The KVSS-II (area under the curve [AUC], 0.88) and YOF (AUC, 0.88) tests showed equal reliability when discriminating against anosmia in the same subjects (p<0.001, by DeLong method). The sensitivity of the YOF test for anosmia was 79.8% and the specificity was 87.2%. The sensitivity of the KVSS-II test was 85.1%, and the specificity was 81.4%. The YOF test has been recognized as an olfactory test to evaluate olfactory impairment under the Korea Workers’ Compensation and Welfare Service since July 2020. To simplify the score interval, a score less than 15 indicates the sense of smell is lost (anosmia); a score exceeding 15 but less than 21 indicates the sense of smell is reduced (hyposmia); and a score exceeding 21 indicates the sense of smell is considered normal (normosmia) [25].
Characteristics of the YOF test and expectations for future use
As mentioned, the YOF test uses PEA as a flavoring agent for the olfactory threshold test instead of n-butanol, which may cause aspiration toxicity. PEA has been used as a raw material for cosmetics for a long time, and its safety for the human body has been verified. It is known that stimulating the trigeminal nerve by chemicals can affect measurement of the olfactory threshold of the olfactory nerve [26]. The characteristic that PEA stimulates the trigeminal nerve less than n-butanol minimizes the disturbance of the olfactory threshold measurement by the trigeminal nerve, enabling more accurate measurement of the function of the olfactory nerve [17]. The sense of smell is a complex sense that is or may be influenced by the environment or emotion, and the feeling of an odor may also affect the detection of an odorant. For example, the threshold for the flavor of food can be different when one is full and when one is hungry [27]. PEA causes a pleasant feeling (pleasant hedonic) in proportion to its concentration. This simple hedonic chemical is used as a flavoring agent for olfactory threshold testing in contrast to other chemicals with a complex hedonic sensation dependent on the concentration. The most commonly used threshold test odorants, PEA (pleasant feeling) and n-butanol (discomfort), have the characteristic of having such a simple odorant. PEA is an odorant that gives a positive feeling in contrast to n-butanol.
In the YOF test, including the olfactory threshold test, each test item consists of 12 steps. This test is expected to shorten the test time from the KVSS-II test, which consists of 16 steps. Croy et al. reported that in a study comparing the reliability of each step in the 16-step and 8-step test using PEA, the 8-step test showed a sufficiently reliable test result with a shortened test time [18]. In another study comparing the reliability of the 16-step and 12-step test using the n-butanol olfactory threshold test, the 12-step threshold test also showed sufficient reliability [28].
The identification test consisted of odorants and sample items carefully selected for the olfactory evaluation of Koreans in the YOF test. A total of 12 odorants consist of 8 odorants for universal cultures and 4 Korean culture-friendly odorants. These 12 odorants are new odorants that do not overlap with the existing KVSS-II identification test odorants except for cinnamon. In addition, each stage is composed of typical examples and has been developed so that there is no wrong answer, even if one smells the scent correctly. As a result, the correct rate of each item in the identification test of the YOF test ranged from 80.7% to 98.6%, and 10 of the 12 odorants showed a correct rate of more than 90% [9]. This result satisfies the 70% correct rate criterion suggested by Doty as a cutoff for the validity of identification test odorants [29]. This cut off criterion has been used as a replacement criterion for odorants when making localized adaptations of the UPSIT [30,31].
When an olfactory source binds to an olfactory receptor in the process of olfactory recognition, the most important influence is the various chemical functional groups of the olfactory source. All 12 odorants of the YOF identification test have one each of the eight major chemical functional groups. It is expected that these characteristics can be utilized to reveal differences in the pattern of olfactory deterioration and help indicating the cause. For example, olfactory dysfunction in neurodegenerative diseases such as Parkinson’s disease or Alzheimer’s disease appears to be most clearly observed in olfactory recognition [32]. If the sensitivity or specificity shown in the loss of smell of these neurodegenerative diseases is different for each chemical group, it could be used as an early diagnostic biomarker.
CONCLUSION
As the understanding of olfaction increases, the importance of olfactory function evaluation is also increasing. The YOF test, a newly developed olfactory function test, was established by reflecting on the olfactory experience of Koreans and has the advantage of using chemicals that have been proven to be safe in the human body. Compared to the existing olfactory test, the YOF test showed an equivalent level of diagnostic utility, and it was also recognized for its usefulness as a diagnostic test for a disability certificate. In addition, representative chemical functional groups are reflected in the properties of odorants for the olfactory recognition test, which is expected to be applied to various diseases accompanied by olfactory dysfunction in future studies.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.18787/jr.2021.00379.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Author Contributions
Conceptualization: Hyung-Ju Cho, Chang-Hoon Kim. Data curation: Jong Gyun Ha. Formal analysis: Jong Gyun Ha. Funding acquisition: Chang-Hoon Kim. Methodology: Hyung-Ju Cho, Jong Gyun Ha. Project administration: Chang-Hoon Kim. Writing—original draft: Hyung-Ju Cho. Writing—review & editing: Chang-Hoon Kim.
Funding Statement
This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the ministry of Science, ICT & Future Planning (NRF-2016M3A- 9D5A01952414). This work was supported by the National Research Foundation of Korea (NRF) Grant funded by the Korean Government (MSIP) (No. 2016R1A5A2008630). This study was supported by the “Team Science Award” of Yonsei University College of Medicine (6-2021-0005).