



INTRODUCTION
Plasmacytoma is a rare neoplasm characterized by uncontrolled proliferation of plasma cells. It can be classified as multiple myeloma (MM), solitary plasmacytoma, or extramedullary plasmacytoma (EMP), depending on its clinical features and morphological characteristics [1]. MM is a neoplastic plasma cell disorder, which usually presents with bone marrow involvement, hypercalcemia, renal failure, and anemia [2]. EMP is a soft tissue tumor characterized by plasma cell infiltration that develops secondary to hematogenous spread [3]. The prevalence of EMP in MM patients is approximately 6%–8% at diagnosis and approaches 10%–30% during the course of the disease [4]. Herein, we describe a rare clinical presentation of EMP involving both maxillary sinuses after complete remission from MM treated with chemotherapy.
CASE REPORT
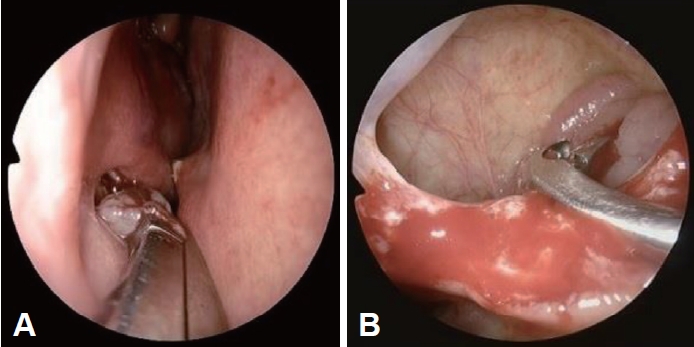
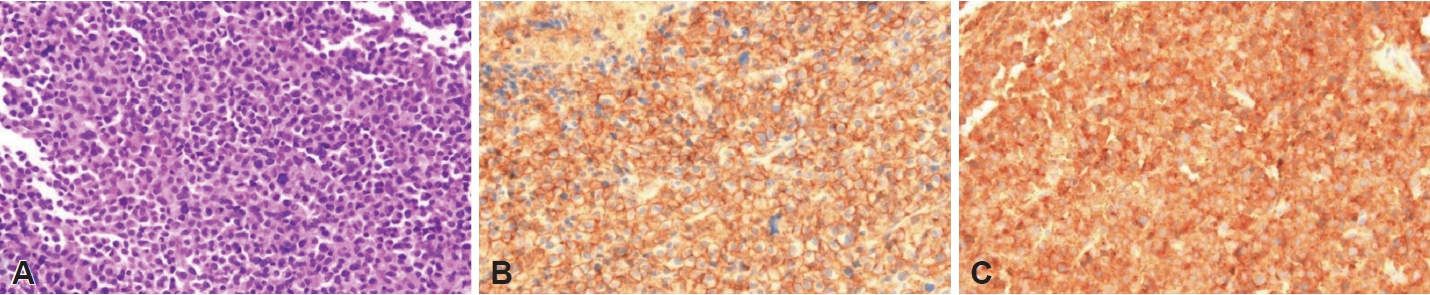
A 73-year-old male patient was referred to our clinic for evaluation of a right nasal cavity mass lesion. He had experienced headaches, posterior nasal drip, and hyposmia for several months and the lesion was identified on computed tomography (CT) at a local clinic. He had been diagnosed with immunoglobulin D lambda MM with multiple intraosseous extramedullary disease 2 years ago. The patient’s MM was classified as stage III according to the international staging system (ISS) and was ineligible for high-dose therapy with autologous hematopoietic stem cell transplantation. He received a nine-course regimen of bortezomib, melphalan, and prednisone (VMP) and achieved complete remission during followup. Our endoscopic examination revealed bulging of the right lateral nasal wall (Fig. 1A). The right middle meatus could not be assessed because the entire nasal cavity was occluded. A paranasal sinus CT scan showed a large expansile enhancing mass with destruction of the right maxillary sinus wall extending to the nasal cavity. An enhancing soft tissue mass was also identified in the left maxillary sinus (Fig. 1B-D). Transnasal endoscopic biopsies of both maxillary sinus masses were performed under general anesthesia (Fig. 2). Histopathologic examination of both specimens showed diffuse infiltration of mature and immature plasma cells with nuclear atypia (Fig. 3A). Immunochemical staining revealed that the neoplastic plasma cells were strongly positive for CD 138 and immunoglobulin light chain (Fig. 3B and C, respectively). These findings were consistent with EMP. On positron emission tomography/CT scan, increased fluorodeoxyglucose uptake was detected in both maxillary sinuses. The patient was classified as stage III according to the ISS. The patient received radiotherapy (total dose, 50 Gy). After 12 months of post-therapy follow-up, the patient exhibited no evidence of residual or recurrent disease (Fig. 4).
DISCUSSION
Plasma cell neoplasia includes various disease groups including MM, plasma cell leukemia, solitary plasmacytoma of the bone, EMP, Waldenstrom macroglobulinemia, primary amyloidosis, light chain deposition disease, and heavy chain disease [5]. EMP is a rare disease defined as the massive infiltration of plasma cells into tissues or organs and can be primary or secondary. Most EMPs develop secondary to MM and appear as masses. Firsova et al. [6] reported the incidence of plasmacytoma as 3.5% to 18% in patients with newly diagnosed MM and 6% to 30% in patients with relapsed disease. The extremely rare cases of EMP that involve both paranasal sinuses present with a maxillary sinus mass. Ours is the first case report of EMP arising from both maxillary sinuses during a complete remission from MM following chemotherapy.
The common clinical features of EMP are associated with soft tissue swelling and nasal symptoms, such as nasal congestion, nasal discharge, and epistaxis. In addition, pain, proptosis, cervical lymphadenopathy, and abducens nerve palsy have been reported [7]. However, these findings are often nonspecific and may lead to misdiagnosed sinonasal malignancies.
Both CT and magnetic resonance imaging can provide valuable information for the diagnosis of EMP. The primary radiographic differential diagnosis for EMP is lymphoma. EMP is more heterogeneous than non-Hodgkin’s lymphoma, with moderate signal intensity on T1-weighted images [8].
The final diagnosis of EMP is confirmed by histopathologic examination. Histologically, plasmacytomas exhibit monotonous proliferation of pure plasma cells in varying degrees of maturation or differentiation within a vascular matrix containing minimal fibrous stroma. On immunohistochemistry, the plasma cells are CD45 and CD20 negative, and express CD138 and epithelial membrane antigen [9]. A monoclonal expansion of kappa or lambda light chains is usually observed, and nearly 70% of plasma cell neoplasms are kappa-positive [10]. In this case, the tumor was positive for CD138 and monoclonal immunoglobulin light chain, which was consistent with EMP.
Surgical resection or radiotherapy are the treatments of choice for primary EMP confined to the sinonasal cavity. Systemic chemotherapy and stem cell transplantation are recommended for relapsed/refractory disease or multiple plasmacytomas [2,11]. This patient had received nine cycles of VMP chemotherapy and achieved complete remission for 1 year. Relapse is a frequent problem for patients with MM and the presence of EMP is linked to a poor prognosis and short survival. Previous studies showed that patients with EMP at relapse had a progression-free survival and overall survival of 9.1 months and 11.4 months, respectively [12,13]. In our case, the EMP originating from both maxillary sinuses was successfully treated by radiotherapy, after considering the postoperative complications and morbidity of complete surgical resection.
In conclusion, although EMP arising from both paranasal sinuses is rare, it should be considered in the differential diagnosis of sinonasal tumors, especially with a history of MM. When it appears impossible to completely resect a locally aggressive EMP in the maxillary sinus, radiotherapy could be considered as primary treatment.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






