



INTRODUCTION
There are many surgical paths to the maxillary sinus. If the lesion lies on the anterior side or floor of the maxillary sinus, surgery featuring a large middle meatal antrostomy is often associated with a limited visual field. Good visibility is essential for the en bloc resection of recurrent lesions, such as inverted papilloma (IP). When approaching the maxillary sinus, the Caldwell-Luc procedure, lateral rhinotomy, midfacial degloving approach, and endoscopic medial maxillectomy are widely used; however, various complications of such approaches are well known.
Recent studies have introduced a prelacrimal window approach (PLWA) to preserve the turbinate and lacrimal apparatus and have found that the prelacrimal or alveolar recess can be accessed [1,2]. Suzuki et al. [3] analyzed the utility of a modified transnasal endoscopic medial maxillectomy (TEMM) approach, which preserves the inferior turbinate and shifts the lacrimal duct medially. Recurrence occurs only in 1 of 51 patients who underwent surgery to remove an IP; the inferior turbinate was preserved without atrophy, and no deformity was observed. Some patients required partial osteotomy of the apertura piriformis or the anterior wall of the maxillary sinus, but the procedure was nonetheless safe and effective.
Simmen et al. [4] used computed tomography (CT) to analyze anatomical variations in the anterior wall of the maxillary sinus and the lacrimal apparatus and suggested that surgeons should evaluate the difficulty of PLWA before surgery. If the distance between the anterior walls of the maxillary sinus and lacrimal duct (D1) was 0–3 mm (type 1), a significant amount of bone resection and temporary dislocation or resection of the lacrimal duct was required to access the anterior wall of the maxillary sinus. Even if a window is created, it is small and compromises full access. When D1 was >3–7 mm (type 2), the sinus was accessible, but partial dislocation of the lacrimal duct may be required. Type 3 D1 (>7 mm) allows easy access to the maxillary sinus. A previous study in Europeans population reported that the frequencies of types 1, 2, 3 were 31.5%, 56.0%, and 12.5%, respectively, thus, the type 2+3 was 68.5%. Lock et al. [5] analyzed 200 CT scans from 100 Chinese patients; the frequencies of types 1, 2, and 3 D1 were 6.5%, 53.5%, and 39.5%, respectively; the ease of the PLWA was 93.0% (type 2+3). Based on these results, it has been suggested that Asians exhibit more paranasal sinus (PNS) pneumatization than Europeans. However, none of the studies evaluated healthy controls.
This study aimed to compare the ease of the PLWA between the patient group and healthy controls and analyze the results for Koreans and those of previous studies. The differences between the patient and control groups and the distribution of types in the Korean population were also evaluated.
METHODS
Subjects
We retrospectively analyzed CT data from 51 healthy controls and 38 patients. Healthy controls were adults (>18 years old) with no history of PNS disease and those without evidence of disease on PNS CT. The patient group included all adults with IP who visited Konkuk University Hospital between 2005 and 2019. We excluded those who lacked anatomical landmarks. PNS CT scans were obtained using a GE Optima 660 platform. The CT scans covered the PNS from the alveolar process of the maxilla to the roof of the frontal sinus. Axial and coronal images were obtained by reconstruction at a slice thickness of 2 mm; the CT parameters were 100 kVp and 65< mA <150 (auto-mA). The study was approved by the Ethical Committee of the Konkuk University Hospital (IRB No. KUMC 2019-08-019-004).
Evaluation indicators
Using the method described in a study by Simmen et al. [4], we identified the coronal plane of the anterior insertion of the inferior turbinate into the frontal process of the maxilla (Fig. 1A). An imaginary line (line 1) was drawn in the corresponding axial plane through the posterior surface of the anterior wall of the maxillary sinus and parallel lines passing through the anterior (line 2) and posterior (line 3) walls of the lacrimal apparatus were drawn. D1 was between lines 1 and 2, and D2 was between lines 1 and 3 (Fig. 1B). Thickness (T) was measured at the midpoint of D1.
Statistical analyses
Statistical analyses were performed using R ver. 3.5 and SPSS ver. 17 software. A paired t-test was used to compare the right and left sides. The Shapiro-Wilk tests was performed to evaluate the normality. Independent t-test was performed to compare D1, D2, and T values between the two groups, and the chi-square test was used to compare groups with D1 >3 mm (type 2+3) and D1 ≤3 mm (type 1).
RESULTS
Demographic characteristics
The mean age was 46.9 and 58 years in the control and patient groups, respectively. The control group consisted of 27 males (53%) and 24 females (47%), and the patient group had 29 males (76%) and nine females (24%) (Table 1). The Shapiro-Wilk tests was performed to evaluate the normality on all measured values and did not show a significance departure from the normality. In normal control groups, the mean D1 was 5.3±1.8 mm, the mean D2 was 32.0±5.0 mm, and the mean T was 4.3±1.6 mm. In the patient groups, the mean D1 of the normal sinus and sinus with IP was 5.12±1.85 mm and 5.07± 1.76 mm, respectively. The mean D2 of the normal sinus and sinus with IP was 31.9±4.9 mm and 30.69±5.77 mm, respectively. The mean T of the normal sinus and sinus with IP was 5.82±2.75 mm and 5.51±2.33 mm, respectively. There are no significant differences observed in D1, D2, T between the sinus with IP and normal sinus (Table 2).
Distribution of types in Koreans
For the entire participant series, the frequencies of types 1, 2, and 3 were 7.8% (11/141), 78.7% (111/141), and 13.5% (19/141), respectively; in the control group, the percentages were 6.9% (7/102), 78.4% (80/102), and 14.7% (15/102), respectively, and in the patient group the percentages were 10.3% (4/39), 79.5% (31/39), and 10.3% (4/39) respectively. There was no significant difference between the two groups (p=0.697) (Table 3).
Distances in the control and patient groups
When the measurements of prelacrimal window in the maxillary sinus medial wall were compared, D1 and D2, did not differ significantly between the control and patient groups. The T of the patient group was significantly greater than that of the control group (Table 4).
Comparison with previous studies
In this study, measured D1 of Korean populations was 5.30± 1.80 mm. And according to a previous study [4,5], D1 was estimated to 6.64±2.36 mm in Chinese populations and 4.24± 2.40 mm in European populations (Table 5).
We also evaluated whether the distributions in the Korean population differed from those of Europeans and Chinese; significant differences were evident. There were only significant differences between Koreans and Europeans and between Europeans and Chinese. In our group, the type 2+3 frequency was 92.2%; meanwhile, the frequencies of Europeans and Chinese patients were 68.5% and 93.0% respectively (Fig. 2).
DISCUSSION
Maxillary sinus lesions may be approached using the Caldwell-Luc technique, lateral rhinotomy, and midfacial degloving. Endoscopic medial maxillectomy has recently become popular because it is less invasive than other methods. However, endoscopic medial maxillectomy may damage the inferior turbinate or lacrimal duct, resulting in complications such as crusting or epiphora. In addition, access to the anterior wall and floor of the maxillary sinus is limited. In 2007, Zhou et al. [1] introduced a technique to preserve the inferior turbinate and lacrimal apparatus. In 2011, Suzuki et al. [3] reported a similar procedure referred to as TEMM, which preserves the inferior turbinate and shifts the lacrimal duct medially, allowing complete resection of maxillary sinus lesions. Simmen et al. [4] suggested that the ease of a PLWA could be determined by measuring the distance between the anterior wall of the maxillary sinus and the lacrimal apparatus, allowing the surgeon to plan an approach. Compared with open approaches, PLWA provides better vision and surgical access to the anterior wall and floor of the maxillary sinus, with lower morbidity and recurrence rates.
In general, it is known that Asian heads have shorter front and rear lengths than those of European. However, in this study, D1 of Koreans and Chinese was measured to be longer than D1 of Europeans. And the type 2+3 frequency was also higher than Europeans. This shows that the difference in head length between Asians and Europeans does not reflect the differences in the anatomical lengths of all organs inside the head. Indeed, looking at the examples of other organs, Moon et al. [6] introduced that the length of the orbital floor did not statistically significantly different between race. Similarly, when looking at this study and the previous study [4,5] together, it can be seen that the length of D1 for Asians is generally longer than D1 for European. More follow-up studies are needed to determine the exact cause of this occurrence.
In our study, the frequencies of types 1, 2, and 3 were 6.9% (7/102), 78.4% (80/102), and 14.7% (15/102), respectively, in the control group and 10.3% (4/39), 79.5% (31/39), and 10.3% (4/39), respectively, in the patient group; no significant differences were observed between the two groups (p=0.697) (Table 3). The T of the patient group was significantly greater than that of the control group. The most common location of IP is the lateral nasal wall, and the second is maxillary sinus, which causes local hyperostosis, resulting in a difference in T [7]. In addition, the T appears to have thickened due to bone changes caused by inflammation.
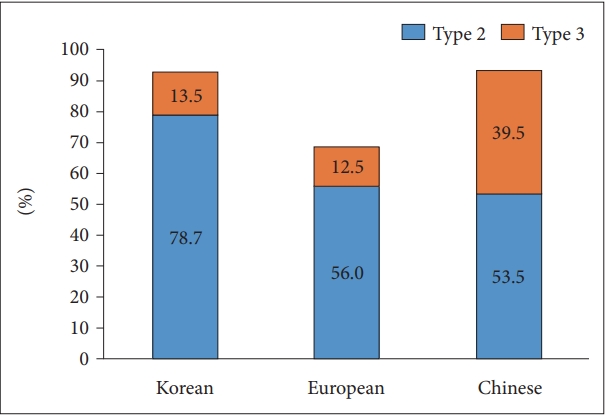
The frequency types in Korean, Europeans, and Chinese populations were 7.8%, 31.5%, and 6.5%, respectively, for type 1; 78.7%, 56%, and 53.5%, respectively, for type 2; 13.5%, 12.5%, and 39.5%, respectively, for type 3 (Fig. 3). In our study, 92.2% of patients were classified as type 2+3; a PLWA is very feasible. The frequencies for Europeans and Chinese were 68.5% and 93.0%, respectively; the PLWA may be more appropriate for Chinese than for Europeans. We found that our results in the Korean population were more similar to the Chinese than European. Therefore, we can suppose that there is high feasibility of PLWA in Northeast asians.
There were some limitations to this study. First, this study include the small number of participants. Further studies are needed in patients with other tumor lesions affecting the anterior wall and floor of the maxillary sinus. Second, despite excluding those who lacked anatomical landmarks, CT images were obtained by reconstruction at a slice thickness of 2 mm, so it had some measuring error. These factors could limit accurate measurement.
In conclusion, D1 and D2 of the patient group did not differ from the control group, and T was greater in the patient group. In the patient group, D1 and D2 were not significantly different between sinus with IP and normal sinuses. The frequency of patients with type 2+3 was similar to that of the control group. The D1 distribution in Koreans was similar to that in Chinese. The ease of a PLWA was 92.2% (type 2+3), which is more similar to that of the Chinese than the European patients. In Korea, when the lesion is the anterior portion of the maxillary sinus, the PLWA technique is recommended more actively.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






