



INTRODUCTION
Obstructive sleep apnea (OSA) is a sleep disorder characterized by repeated upper airway collapse during sleep. Some studies have demonstrated the effects of sleep positions on the severity of OSA [1–10]. Worsening of OSA occurs in supine positions rather than non-supine positions because of more frequent upper airway collapse. Based on these findings, the concept of positional OSA was first introduced by Cartwright [11] as apnea-hypopnea index (AHI) being at least 50% greater in supine positions than in non-supine positions. According to the American Academy of Sleep Medicine (AASM), positional OSA is defined as a lower AHI in the non-supine position than in the supine position [12]. On the contrary, the influence of the lateral decubitus sleep positions on OSA has not been well investigated. Several studies have tried to analyze the effect of lateral sleep positions [2,5,6,8–10], but very few studies have focused on specific effects of right and left lateral decubitus position (RLDP and LLDP) on sleep parameters [6].
Polysomnography (PSG) is generally regarded as gold standard tool for analysis of sleep disorders, but the clinical efficacy of peripheral arterial tonometry (PAT) using the Watch-PAT device (Itamar Medical, Caesarea, Israel) has also been well validated [13,14]. The attached body position sensor of the WatchPAT contains three-axis accelerometer, allowing detection of not only AHI, arousal, and sleep stage but also the sleep position. Since overnight PSG is expensive and time-consuming, WatchPAT is now widely used as an alternative examination technique in patients with sleep disorders.
In this study, we investigated the effects of lateral decubitus positions on severity of OSA and the association between sleep parameters and RLDP/LLDP using WatchPAT device.
METHODS
Patients
We retrospectively reviewed the medical records of 58 patients who had undergone surgical interventions for treatment of OSA after preoperative WatchPAT analysis from January 2014 to December 2016 in one tertiary referral center. Among them, 38 patients who slept more than 10 minutes in both RLDP and LLDP were included in this study for the comparative analysis of two positions. Nasal endoscopic examination, acoustic rhinometry, and computed tomography (CT) scan were performed for analysis of anatomical variations. We chose patients who had undergone surgical interventions because their clinical information was more thoroughly investigated and documented than that of patients who had not. This study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 1711-021-897).
WatchPAT
Overnight WatchPAT examination was performed in all patients. The automatically analyzed WatchPAT parameters included snoring level, snoring threshold, PAT AHI (pAHI), PAT respiratory disturbance index (pRDI), arterial oxygen saturation, and body position. The pAHI and pRDI were calculated separately in accordance with the body position. The body position during sleep was divided into supine, prone, right and left from the WatchPAT software using a signal from the position sensor. To investigate the effects of lateral decubitus position, the differences in pAHI and pRDI between RLDP and LLDP were calculated for all patients.
Statistical analysis
All statistical analyses were performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). All results with continuous values are expressed as mean±standard deviation. Body mass index (BMI) and the difference in each sleep parameters between the two lateral decubitus positions were analyzed using Pearson’s correlation coefficient. Analysis of variance (ANOVA) and post-hoc test was carried out for evaluation between the body positions. The difference in each sleep parameters between patients with right and left-sided deviated nasal septum (DNS) was analyzed using Mann–Whitney U test. Statistical significance was defined as p-value<0.05.
RESULTS
The patients were comprised of 36 males and 2 females. The mean BMI was 26.18 kg/m2. Nasal endoscopic examination and CT imaging revealed DNS to the right side in 18 patients and to left side in 20 patients. The type of DNS was classified according to Guyuron’s classification [15], but the side of DNS was only assessed in this study. All patients underwent surgical interventions for treatment of OSA (septoplasty in 36 patients, soft palate surgery in 35, and tongue base surgery in 3) (Table 1).
WatchPAT data
The mean value of pRDI and pAHI during the total sleeping hours was 26.68±15.23 and 21.31±17.03, respectively. The pRDI and pAHI were significantly higher in supine position than in non-supine positions. However, the sleep position percentage was significantly higher in supine position, RLDP, and LLDP than in prone position (Table 2). Since the study only included patients who slept sufficiently in lateral decubitus positions, above finding might be the selection bias.
Correlation between body mass index and sleep parameters in right lateral decubitus position and left lateral decubitus position
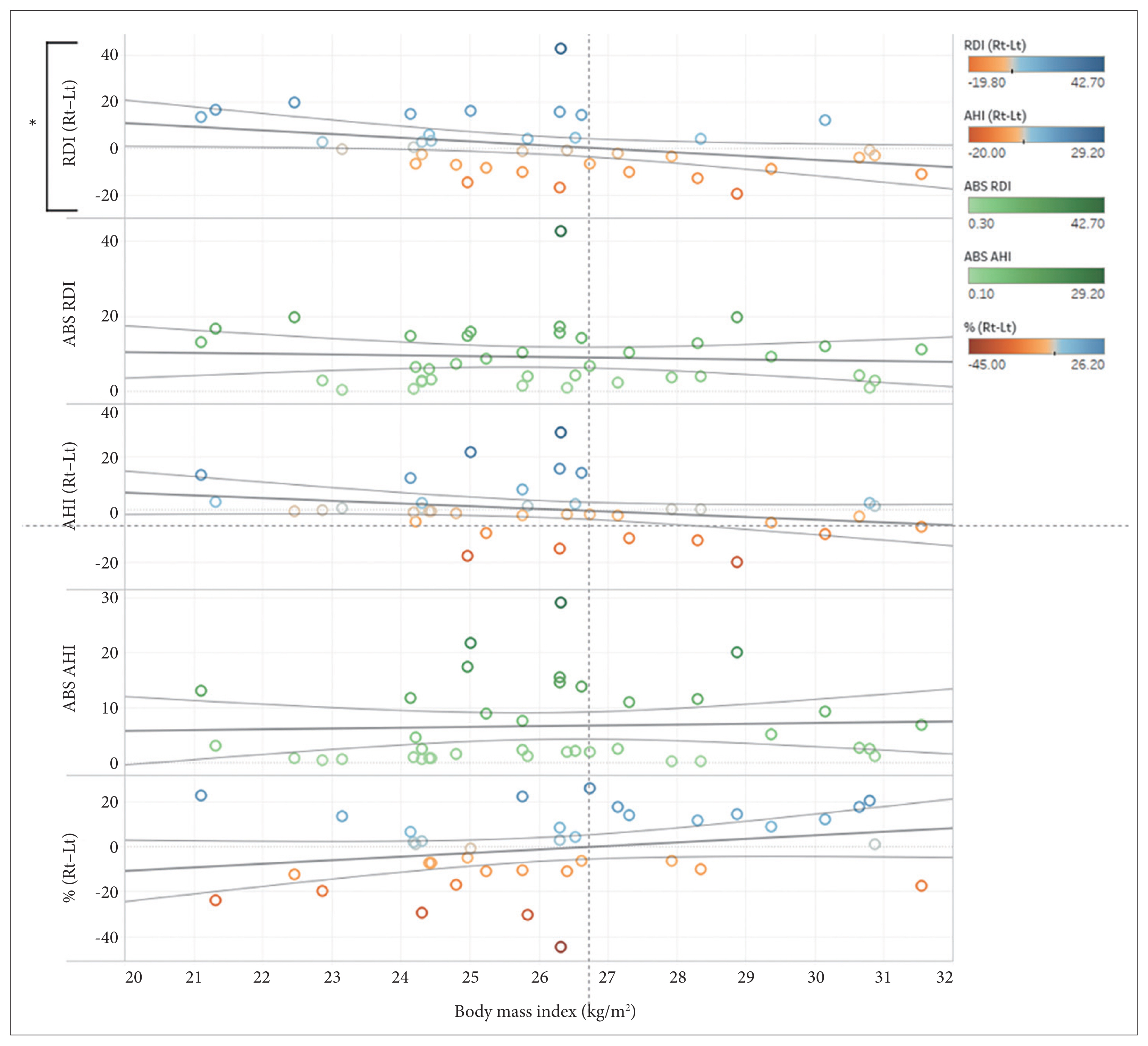
The correlation between BMI and pAHI or pRDI in RLDP and LLDP was analyzed in 38 patients. The absolute value of the difference in pAHI and pRDI between the two lateral decubitus positions was not correlated with BMI. There was also no correlation between BMI and the difference in pAHI between RLDP and LLDP. However, the difference in pRDI between RLDP and LLDP (Rt–Lt) was significantly correlated with BMI (p=0.038, R2=0.115) (Fig. 1). The higher BMI patient showed, the higher pRDI was detected in LLDP than RLDP.
Effect of lateral decubitus sleep position
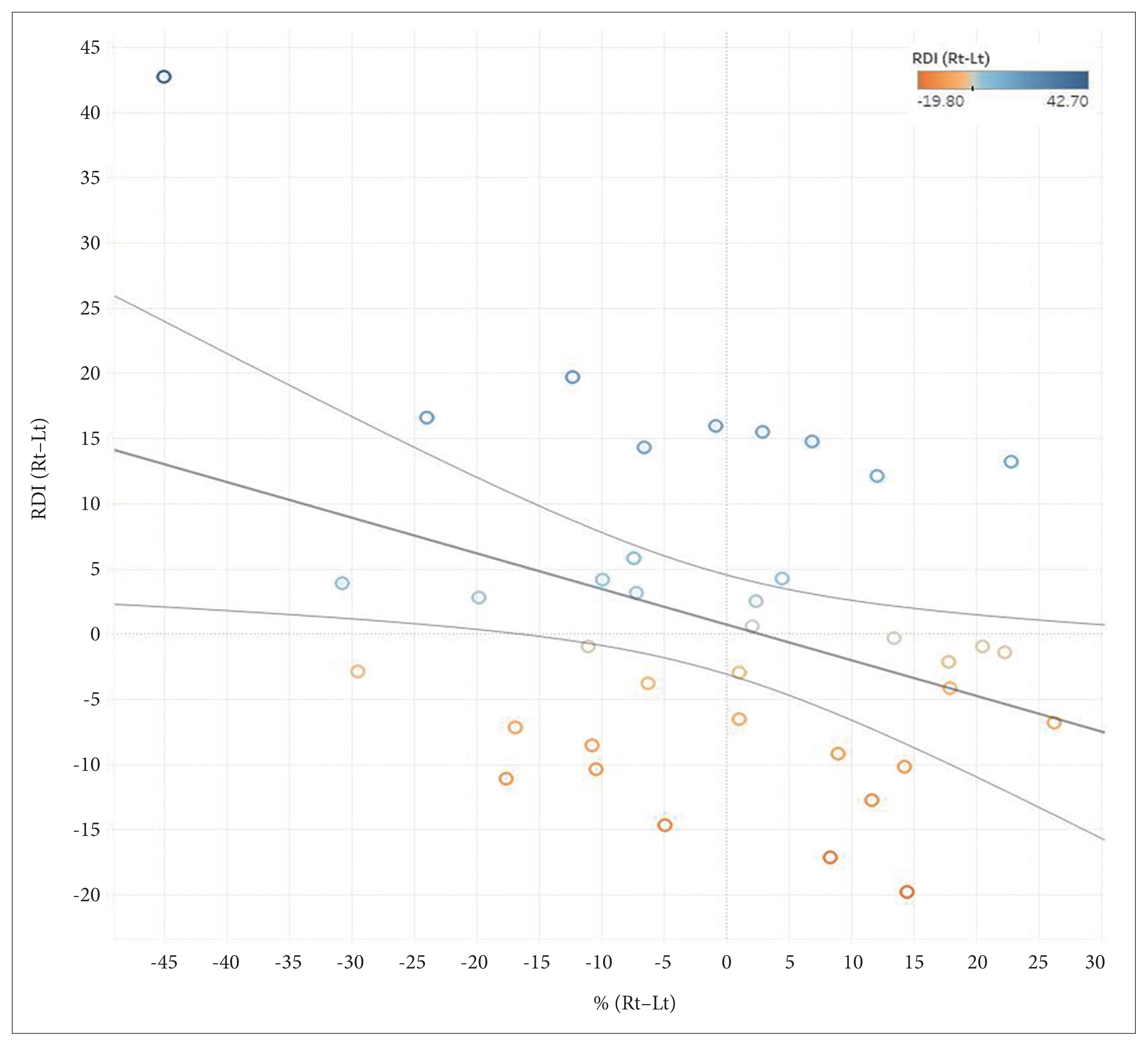
The correlation between sleep position percentage in each lateral decubitus position and sleep parameters was analyzed. The value obtained after subtraction of the sleep position percentage from the RLDP to LLDP showed significantly negative correlation with the value obtained after subtraction of pRDI from RLDP to LLDP (p=0.023, R2=0.135) (Fig. 2). The decubitus position in which patients slept for longer period of time was associated with lower pRDI. However, there was no statistically significant correlation between the difference in pAHI and sleep percentage (p=0.066, R2=0.091) (Fig. 3).
Differences in sleep parameters between patients with right and left-sided deviated nasal septum
The sleep parameters in each lateral decubitus position were compared between patients with right and left-sided DNS. No correlation was found between the differences in pRDI, pAHI, or sleep position percentage in two lateral positions and DNS side (Fig. 4).
DISCUSSION
We used WatchPAT data and patient demographics to identify variables that may influence sleep parameters in RLDP and LLDP during sleep. The association between BMI and various sleep parameters in each lateral decubitus position was investigated. Although the association between BMI and the severity of OSA has been proven in many previous studies [16,17], association with the lateral decubitus position was not well known. We primarily tried to focus on the anatomical factors related to higher BMI-induced lateral obstruction in each lateral decubitus sleep position. However, the absolute value of the difference in pAHI between RLDP and LLDP showed no association with BMI. Interestingly, patients with higher BMI showed higher pRDI in LLDP. There have been several studies claiming of the weak or no correlation between AHI and BMI [18,19]. One study has demonstrated no correlation between BMI and AHI, although neck and abdominal fat and neck circumference were more effective in predicting AHI [18]. Unlike AHI, RDI includes respiratory effort-related arousals, and thus indicates not only apneas or hypopneas but also increased respiratory effort. Therefore, it can be hypothesized that LLDP might induce more increased respiratory efforts than RLDP. Respiratory effort-related arousals are known to be associated with elevation of cardiac sympathetic tone. Patients with higher RDI may be exposed to increase in cardiac sympathetic modulation [20]. In some studies, patients with chronic heart failure are recommended to avoid sleep in LLDP [21,22]. This is believed to be associated with lung diffusion impairment or further hemodynamic compromise induced by increased heart dimensions. Moreover, the cardiac vagal activity is greater in RLDP [23]. Considering strong association between obesity and heart failure [24], such findings may well explain the worsening of pRDI in LLDP in patients with higher BMI.
In contrast, another study revealed that in patients with moderate to severe OSA, the AHI, not RDI, was higher in left-sided sleep positions [6]. The authors explain that such results might be due to the presence of concomitant patent foramen ovale with OSA or the reduced venous return resulting from greater shifting of the mediastinum in LLDP than in RLDP.
Many previous studies have explained about the possible mechanism of preferred sleep positions. Possible explanations of people avoiding supine position include increased energy required for respiratory movements of the rib cage [25], loss of flexibility of spine as people age [26], and uncomfortable feeling of enlarged heart beating on left chest wall [21]. However, there has been scarce report on explaining which specific side position is preferred among OSA patients, and which factor is associated. Our study has revealed that patients try to sleep in lateral decubitus position which derives lower pRDI. The difference in sleep position percentages between RLDP and LLDP showed negative correlation with the difference in pRDI. Patients slept for shorter amount of time in certain position with higher pRDI. This might be a protective strategy to reduce apnea events, which are closely related to many forms of cardiovascular diseases including hypertension, stroke, heart failure, etc. Such findings can be applied to positional therapy in treating OSA, encouraging patients to sleep more in certain lateral decubitus position.
Although PSG has been regarded as the gold standard tool for diagnosis of sleep disorders, WatchPAT is now widely used as an alternative due to its convenience and cost-effectiveness. One meta-analysis of 13 studies showed that WatchPAT data consistently demonstrated a high degree of correlation with PSG results [14]. Regarding patient’s sleep positions, they also found 90% agreement between the WatchPAT device and video recording. The snoring and body position sensor in WatchPAT encloses a microphone and a 3D accelerometer together to acquire the spatial body orientation relatively to the vertical gravity [27].
From preliminary literature review [28–35], we hypothesized that the side of DNS may contribute to the occurrence of apnea or hypopnea events in different lateral decubitus positions. We analyzed endoscopic examination findings, acoustic rhinometry results and CT scan. Patients with severe OSA reportedly showed smaller minimal cross-sectional area in acoustic rhinometry than those with mild or moderate OSA, thus the minimal cross-sectional area was also assessed as well as resistance and volume [35]. Acoustic rhinometry was performed at sitting position before and after administration of nasal decongestant. Then, we calculated the resistance in lateral decubitus position based on the hypothesis that the mucosa of the decubitus side may be swollen while the opposite side of nasal cavity being decongested. However, none of the acoustic rhinometry parameters showed any correlation with sleep parameters in either of the lateral sleep positions. Additionally, the side of DNS evaluated from endoscopic and CT findings also showed no correlation with sleep parameters. Many studies have revealed that septoplasty may improve patients’ quality of life [33,34] or sleep parameters such as the RDI and AHI [29,31]. We tried to analyze the effect of septoplasty on sleep parameters in each lateral decubitus positions, but only few patients (4 of 38 patients) could be assessed due to limited postoperative WatchPAT data and insufficient amount of sleep in lateral decubitus positions.
This study is based on retrospective chart review, which leads to limited patients’ clinical information. We only included OSA patients who had undergone surgical interventions to obtain as much clinical information as possible through preoperative examination findings. For this reason, the study population may not well represent general characteristics of OSA patients, including those requiring continuous positive airway pressure (CPAP) or mandibular advancement devices (MAD) instead of surgical interventions. Moreover, the male to female ratio was 18 to 1, indicating that being male could have affected the results. Mean value of BMI in our study was 26.18±2.63 kg/m2, showing relatively lower values than other studies on OSA. Ethnicity might be the contributing factor, since Asians are known to show lower BMI than other races [36,37]. Therefore, further investigations are needed to clarify our results.
In conclusion, our study revealed that patients with higher BMI showed worse pRDI in LLDP than in RLDP. Patients with higher pRDI in certain lateral decubitus position slept for shorter amount of time in one position. The side of the DNS showed no correlation with sleep parameters. Therefore, to accurately evaluate OSA patients, sleep parameters should be evaluated not only in supine and non-supine positions but also in RLDP and LLDP.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






