



INTRODUCTION
Of all the sinuses, the maxillary sinus stands the most diseased. This can be attributed to its pyramidal shape which makes access to its anterior and medial wall difficult, thereby leading to residual disease. Inverted papillomas, although relatively uncommon, are diagnosed in about 0.5%ŌĆō4% of operated nasal tumours [1]. Among these, the most common site of origin of tumour remains the maxillary sinus [2]. Their high rate of recurrence is a harrowing problem for surgeons which makes its complete removal inevitable. Inverted papillomas have a tendency to invade surrounding bone which makes drilling out diseased bone necessary. Although several advanced techniques have been developed to clear maxillary sinus disease, the efficacy of these remain questionable. This can be attributed to the difficulty in access that most techniques accompany, leading to suboptimal clearance. The current gold standard for the treatment of maxillary sinus inverted papillomas remains to be endoscopic medial maxillectomy. Recent modifications to this technique such as the prelacrimal recess approach have provided improved access to the different recesses of the maxillary sinus [3]. When the sinus pathologies extend anteromedially, usage of angled instruments and endoscopes becomes imperative. However, these pose a problem of not providing adequate space and reach within a single nostril for manipulation and sharp dissection. Our technique describes a modification to transseptal approach described in the past [4] to access inverted papillomas with anteromedial origin and involvement of inner aspect of anterior wall of maxillary sinus.
CASE REPORT
A 54-year-old male presented with right sided nasal block and facial pain. He had similar complaints in the past and was diagnosed to have inverted papilloma for which endoscopic surgery was done twice, once in 2015 and later in 2019. Diagnostic nasal endoscopy was performed which revealed a polypoidal mass filling the nasal cavity on the right side (Fig. 1). Contrast enhanced magnetic resonance imaging of paranasal sinuses revealed an enhancing mass with a distinctive convoluted cerebriform appearance involving lateral wall of nasal cavity extending into maxillary ostium and antrum (Fig. 2).
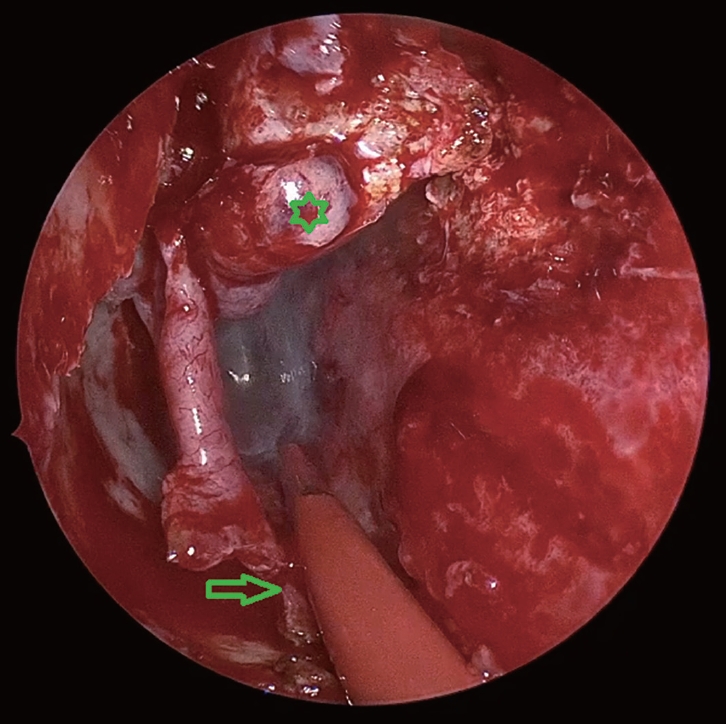
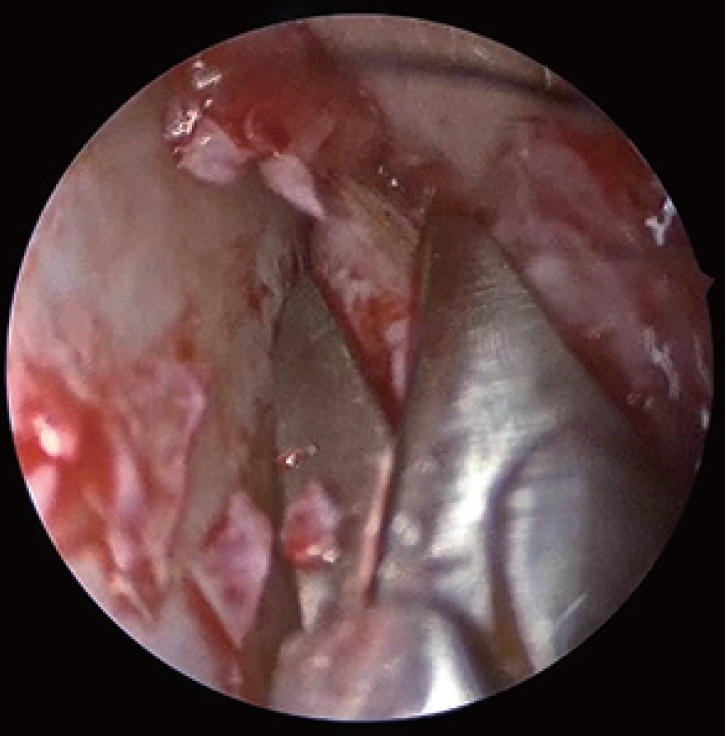
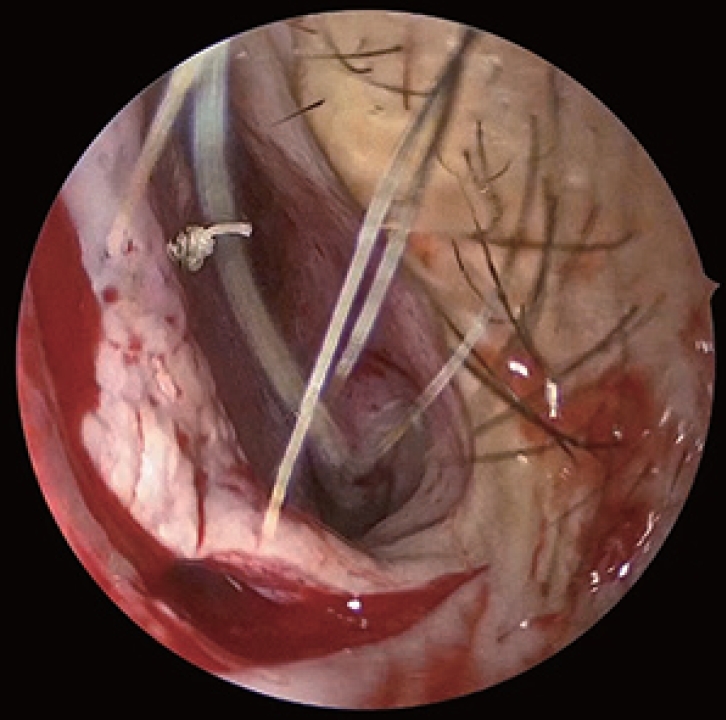
Surgical Technique: Surgery was performed under general anesthesia. Merocel┬« (Medtronic Xomed Inc., Jacksonville, FL, USA) soaked in adrenaline solution (1:1000) was used for local vasoconstriction. On the right side, minimal remnant of uncinate was removed. Following maxillary antrostomy, an incision was made anterior to the inferior turbinate and extended along the floor of the nose posteriorly (Fig. 3). The flap was then elevated exposing the entire lateral wall of the nose (Fig. 4). A 3 mm gouge was used to excise bone anterior to the nasolacrimal duct in a careful manner so as to avoid injury to the duct. The nasolacrimal duct was identified and transposed medially. This provided access to the anterior part of the maxillary sinus where the tumour remained hidden. Using burrs (Sinus Burr 35k, Karl Storz, Tuttlingen, Germany), the bone was drilled opening up the medial wall of the maxillary sinus. The visualised part of the tumour was removed using angled instruments (Heuweiser Forceps, Karl Storz, Tuttlingen, Germany). To gain access to the anteromedial wall and medial buttress, a hemitranfixation incision is made in the contralateral nasal cavity (left side) at the mucocutaneous junction. This incision was extended posteriorly, horizontal along the superior part of nasal septum beneath the nasal roof (Fig. 5). Mucoperichondrial and mucoperiosteal flaps were elevated on the contralateral side and folded posteroinferiorly. The flap falls downwards, allowing space for instrumentation. From the ipsilateral side, a needle (Ethilon 3-0, Ethicon, Johnson and Johnson, Piscataway, NJ, USA) was passed through the septum, corresponding to the opening made on the medial wall of maxillary sinus (Fig. 6). Once the needle pierced beyond the septum on the contralateral side, a cruciate incision was made on the cartilage (0.3 cm├Ś 0.3 cm) (Fig. 7). Curved instruments (Rad Blades 15, 40 and 60 degree, Medtronic Xomed Inc., Jacksonville, FL, USA) of the powered debrider (Medtronic Xomed Inc., Jacksonville, FL, USA) were introduced through this incision providing access to the entire anterior wall of the maxillary sinus on the diseased side (Fig. 8). After tumour removal, the bone underneath its attachments was also drilled using a variety of angled burrs (The DrillCut-X┬« II-35 Handpiece with 35k Sinus Burrs, Karl Storz, Tuttlingen, Germany) in the range of 15┬░, 40┬░and 60┬░ (Fig. 9). 3-0 Vicryl RapideTM (Vicryl Rapide, Ethicon, Johnson and Johnson, Piscataway, NJ, USA) with a knot at one end [5] was used for septal suturing after replacing the mucoperichondrial and mucoperiosteal flaps (Figs. 10 and 11). The lateral wall flap was repositioned and the inferior turbinate was sutured anteriorly. Follow up period showed no crusting, perforation or epiphora. There were no signs of recurrence after a follow up period of one, three and six months. Due to drilling of bone, some degree of maxillary contracture was observed.
DISCUSSION
In conditions such as inverted papilloma, it remains crucial to remove the tumour completely along with its underlying bone, as it houses microscopic cell rests that can lead to tumour progression [6]. However, it is the anatomy of the maxillary sinus that restricts optimum removal, increasing the recurrence rate due to residual disease. Hence based on the location and extent of tumour, an ideal surgical procedure should be chosen. Previously, Caldwell-Luc surgery and various open surgical procedures such as lateral rhinotomy and mid facial degloving were developed to provide access to the hidden buttresses of the maxillary sinus. These procedures are associated with some degree of morbidity and cosmetic deformities postoperatively. It also has limitations of providing restricted access and disruption of natural barriers of nose and paranasal sinuses. At present, the most common method to treat maxillary sinus inverted papillomas remains to be medial maxillectomy. Recent advances include intranasal endoscopic prelacrimal recess approach [7], however, the origin of tumour from the anteromedial wall of the maxillary sinus may remain hidden. Moreover, it remains difficult to use curved instruments in a single nostril to expose the sinus adequately. The concept of transseptal approach has been described in the past. The two-surgeon technique proposed by Douglas and Wormald [8] suggests to place a mucoperichondrial incision in the opposite nostril, remove part of bony septum and to make a mucoperichondrial incision on the side of lesion to allow access of angled instruments. This is the original technique wherein a second surgeon enters the nostril on the opposite side and through the septum introduces instruments to the ipsilateral side facilitating tumour dissection and manipulation. In this a hemi transfixation incision and superior incision are not made at the septum which will otherwise interfere with free manipulation using instruments, especially drills. Our technique modifies the original method by creating an additional incision at the superior aspect giving the advantage of having free, non-interfering access to the nasal septum. This has an additional advantage of helping to avoid accidental injury to the flap. Inverted papillomas in addition tend to invade the Haversian system of bone which warrants drilling of the bone underneath so as to avoid recurrence. In our case described, involvement of the anteromedial aspect of maxillary sinus (the medial buttress of maxillary sinus), access with a drill burr with any angulation would be impossible unless we come from the contralateral side. This is made possible by our modified transseptal approach. Cadaveric studies by Harvey et al. [4] have proved that transseptal approach improves angulation and dissection. Another cadaveric study by Ramakrishnan et al. [9] showed that a modified transseptal approach helped in providing access in the anterior and lateral direction. Dean et al. [10] also described transseptal approach to access tumours previously considered accessible with only external approaches. The need for transseptal surgery must be kept in mind while planning surgery. Once the origin of the tumour has been delineated, the tumour can be resected in a step wise manner. The morbidity associated with this technique remains minimal. Our experience shows that this modification of transseptal technique is a useful tool in adjunct to endoscopic medial maxillectomy and prelacrimal approach to access hidden areas of the maxillary sinus. It appears to provide similar access as that of an open access approach without the associated morbidity such as alar retraction and facial numbness.








 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






