



INTRODUCTION
The incidence of tonsil cancer has been increasing, which can be attributed to a growing proportion of diagnoses associated with infection by the human papillomavirus (HPV) [1]. Because HPV-positive oropharyngeal squamous cell carcinoma (OSCC) is more responsive to chemoradiotherapy than HPV-negative OSCC [2]. Cases of HPV-positive OSCC are associated with more favorable outcomes than those occurring in the absence of HPV infection [3].
Fifteen to twenty percent of oropharyngeal carcinomas develop distant metastases that most commonly involve the lung, liver and bone, and some retrospective reviews have reported that metastases with HPV-related disease are more likely to include unusual sites [4]. As the cavernous sinus involves cranial nerves III to VI, patients with cavernous sinus metastasis could demonstrate symptoms of acute onset diplopia, ptosis and paralytic strabismus.
Few authors have previously reported metastasis to the cavernous sinus from head and neck cancer, and especially, few Asian cases have been reported. We present a patient with diplopia, ptosis and paralytic strabismus caused by a cavernous sinus metastasis who was previously diagnosed with HPV-positive OSCC.
CASE REPORT
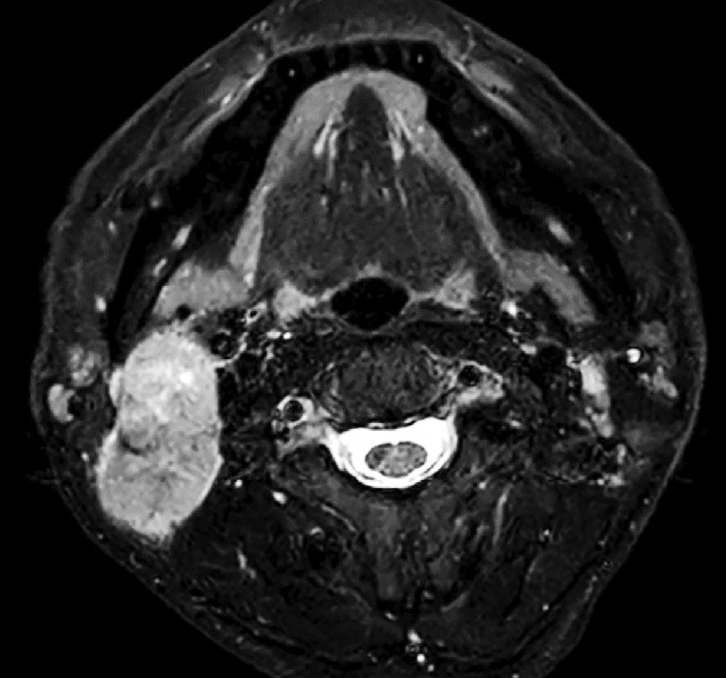
A 59-year-old male ex-smoker (30 PY) who had a six-month history of an enlarging right neck mass associated with neck pain and dysphagia was referred to the head and neck surgery clinic. He was diagnosed with HPV-positive squamous cell carcinoma with neck metastasis (T1N1M0) after biopsy and imaging studies including magnetic resonance imaging (MRI) (Fig. 1). He underwent right palatine tonsillectomy and right modified neck dissection.
After surgery, his pathological staging was modified to pT2N1 (American Joint Committee on Cancer [AJCC] 8th) with extranodal extension to the right 2A lymph nodes and with a close resection margin. The patient received adjuvant 5,940 cGy in 27 fractions to the primary site and ipsilateral neck. Adjuvant concurrent chemotherapy consisted of intravenous cisplatin given as a loading dose of 164 mg/m2, which was started on the first day of radiotherapy, but only one more identical dose of cisplatin was given because the patient was reluctant about continuing chemotherapy.
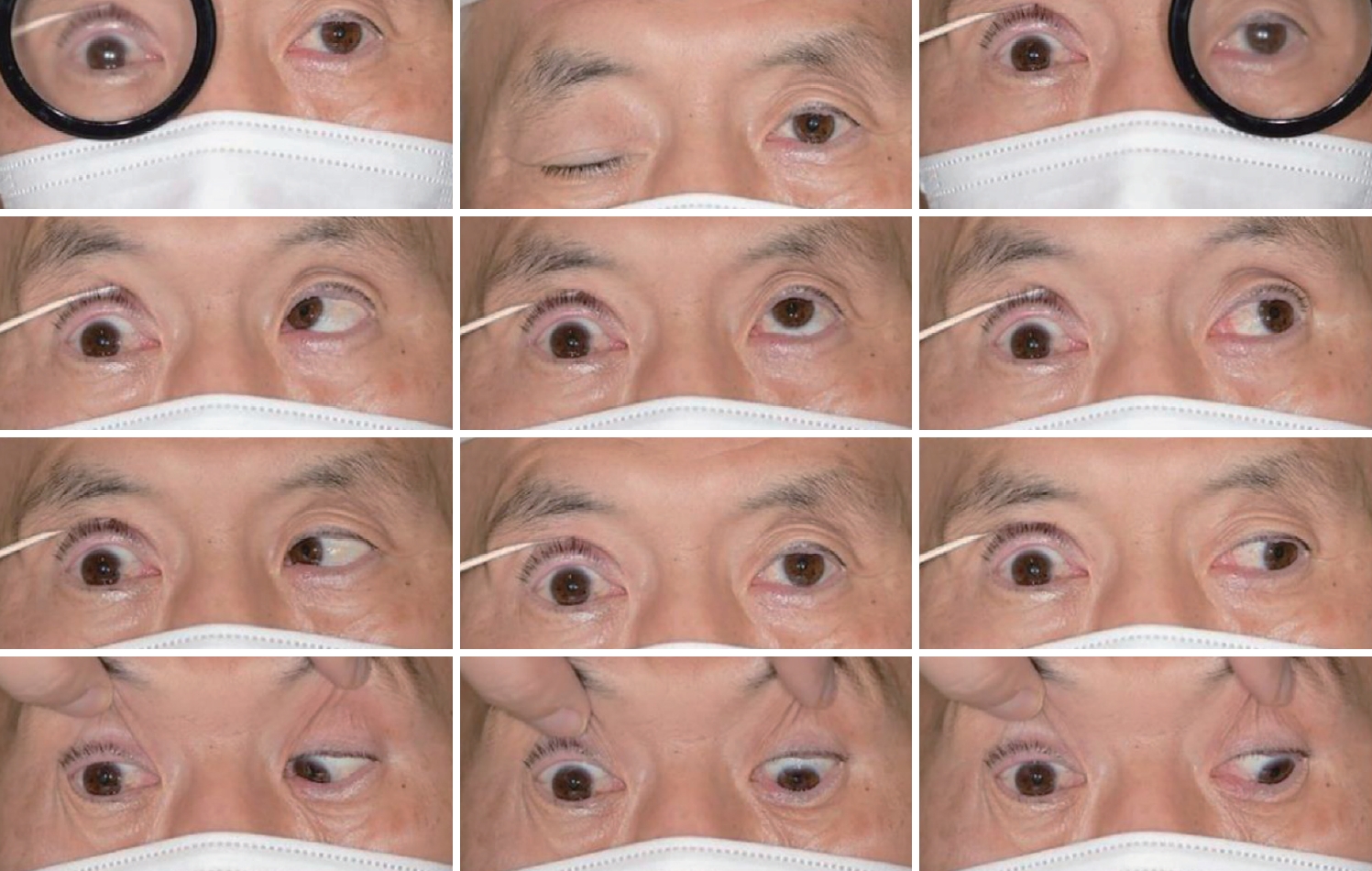
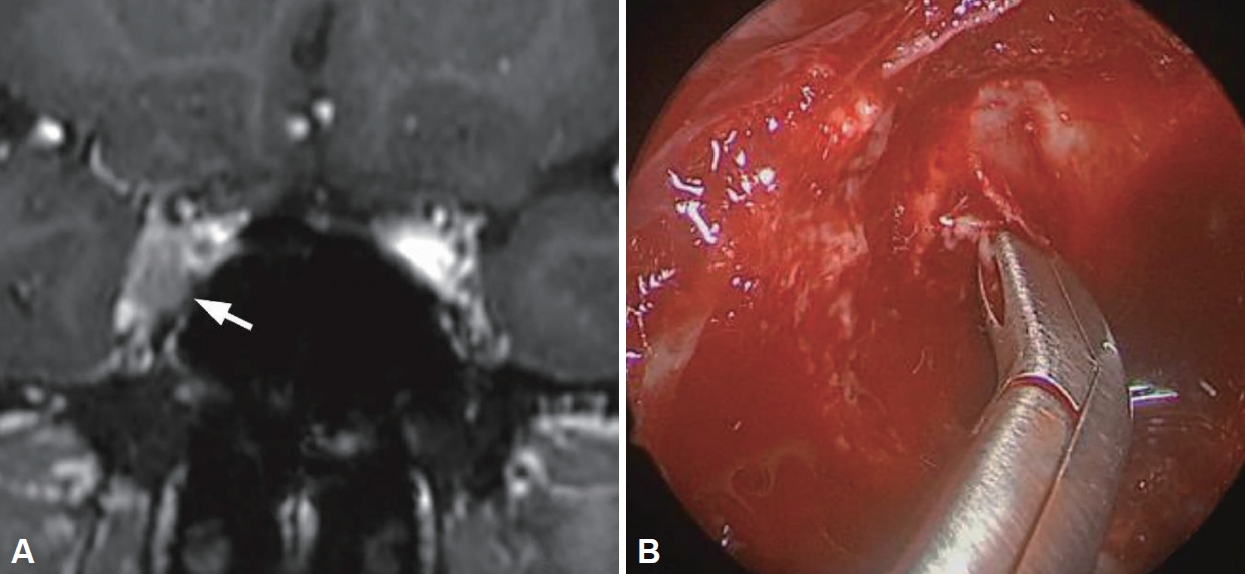
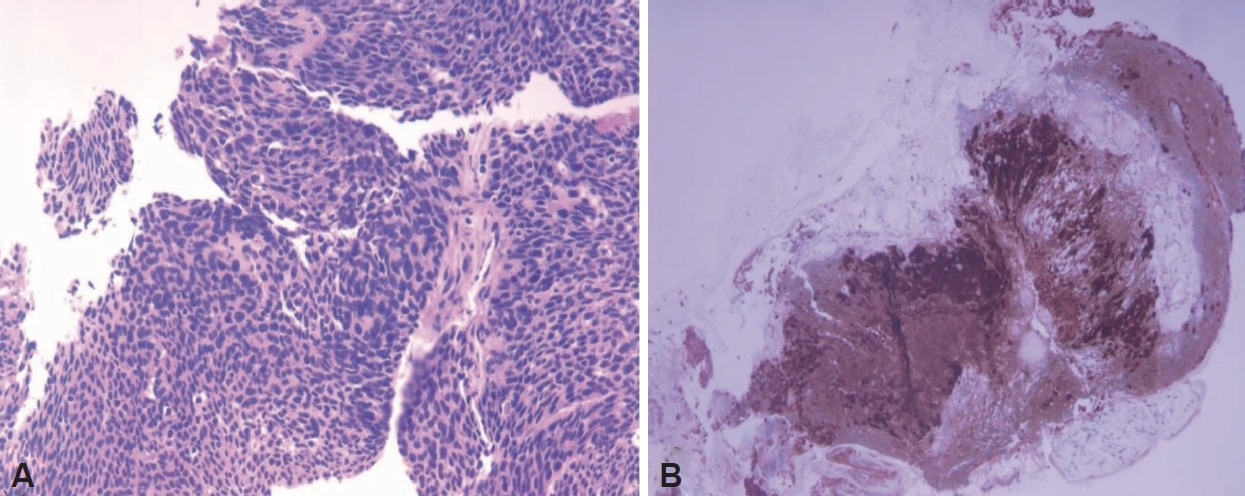
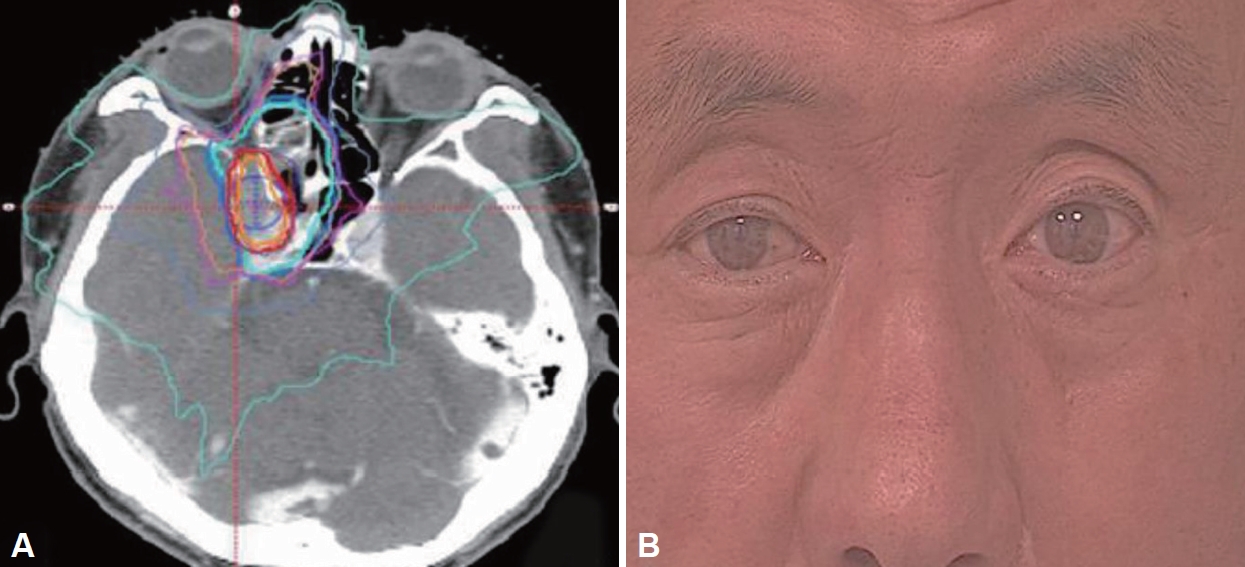
Five months after completing the surgery and adjuvant chemoradiotherapy, the patient visited the emergent department because of complete ptosis and paralytic strabismus of the right eye (Fig. 2). Physical examination revealed right-sided cranial nerve III and VI palsy. MRI showed a mass-like lesion in the right cavernous sinus (Fig. 3A). Because cavernous metastasis from tonsil cancer rarely occurs, we prescribed a total of 12 administrations of high dose intravenous methylprednisolone 250 mg 4 times per day with 3 days to rule out neuritis or Tolosa Hunt syndrome. After steroid therapy, however, the ptosis and diplopia did not resolve, so we decided to perform an endoscopic biopsy for the cavernous sinus lesion. After ethmoidectomy and large sphenoidotomy, we performed the biopsy under image guidance (Fig. 3B). Results from the biopsy confirmed metastasis of HPV-positive squamous cell carcinoma (Fig. 4). The patient received an additional 6,000 cGy in 20 fractions to the right cavernous sinus, and the patient’s ptosis and diplopia improved within one month (Fig. 5). He is planned to have regular follow-ups in the otolaryngology, and radiology departments, and his recent 12 months follow up of neck CT scan showed no evidence of recurrence.
DISCUSSION
This case is unusual; he had HPV-positive tonsil cancer that metastasized to the cavernous sinus without any other distant metastases to the common locations. Very few cases of OSCC metastasis to the cavernous sinus have been reported in the English literature [5-7]. Physicians must maintain a high index of suspicion in patients with a history of malignancy who present with symptoms involving the cavernous sinus. In this situation, detailed physical examinations and imaging studies to investigate a potential etiology must be performed. If imaging studies, such as MRI, reveal the possibility of a cavernous metastasis, endoscopic biopsy could be performed [8].
When the lesion is situated medial to the internal carotid artery, an endoscopic endonasal approach would be simple and safe. However, if the lesion is lateral to the internal carotid artery, an endoscopic transorbital approach could be another surgical option [9]. Because aggressive manipulation could cause permanent nerve paralysis, sharp dissection and small multiple biopsies are suggested when performing the biopsy [10].
Although the exact mechanisms or pathways to the cavernous sinus from the oropharynx have not been revealed, hematogenous metastasis is the most reliable theory because of the high vascularity of the cavernous sinus. Therefore, the overall prognosis is likely to be poor; the expected mortality is 75% to 85% within two years [11].
Despite the patient’s overall poor prognosis, physicians must confirm whether the lesion is a metastasis or a primary tumor. In our case, we promptly performed an endoscopic biopsy, and the patient received early palliative radiation therapy, which allowed complete recovery of the cranial nerve palsies and improved the quality of life for our patient with a poor prognosis.
In conclusion, cavernous sinus metastasis from oropharyngeal carcinoma must be considered in cases of cranial nerve palsies involving the cavernous sinus. Prompt endoscopic biopsy will provide accurate information about prognosis, and proper treatment, such as adjuvant radiation therapy, could improve the quality of life.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






